
What is aphakia?
Aphakia (a, privative, pakos, lens) means absence of crystalline lens from the patellar fossa of the eye. In the majority of the cases the lens has been removed by operation, sometimes it has been lost through a perforating wound, it may be absent as a congenital defect or it may be displaced from the pupil by dislocation.
An aphakic eye is usually strongly hypermetropic; in the absence of crystalline lens , other things being normal, parallel rays of light are brought to a focus about 31mm behind the cornea. While the average antero-posterior diameter of the eye is only 23 to 24 mm. Optical principle is to correct the error by convex lenses of appropriate power, so that the image is formed on the retina. Modalities of correcting aphakia include.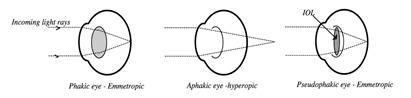
- Spectacles
- Contact lenses
- Intra ocular lenses
- Refractive corneal surgery
SPECTACLES: Spectacle prescription had been the most commonly employed method of correcting aphakia in the past. However, presently, use of a aphakic spectacles had been markedly decrased. Although there is some advantages of spectacle like, it is cheap, easy and safe method of correcting aphakia, but spectacle lenses produce the most disturbing visual problems for the wearer. Fortunately, most of the problems due to aphakic spectacles can be minimized, if not completely solved, by the careful selection of aphakic lenses and frames.
Inherent optical defects of convex lenses which go unnoticed in lenses of low power become so noticeable in high plus lenses as to cause a number of problems for the wearer. The problems include the following:
- Increased retinal image size
- Decreased field of view
- Presence of a ring scotoma
- Increase in ocular rotations
- Increased in lens aberrations
- Motion of object in th field of view
- Appearance of the wearer
- Demand on convergence
- Gullstrand’s schematic emmetropic eye has a refracting power of +58.64D and an anterior focal length of 17.05mm, while the aphakic schemetic eye has a refractive power of +43.05D and an anterior focal length of 23.23 mm. if a correcting spectacle lens is placed at the anterior focal point of the eye, the size of the retinal image is directly proportional to the anterior focal length and inversely proportional to the refracting power of the eye. That is Retinal image size in aphakia / retinal image size in emmetropia = 23.33/17.05 = 58.64/43.05 = 1.36 or an increase in retinal image size of 36%. If the correcting lens is placed at a vertex distance of 12 mm rather than at the anterior focal point of the eye, the required power would be then +10.31D. the retinal image size for this aphakic eye would 1.22 times larger than the retinal image of the schematic emmetropic eye, an increased of 22%. In bilateral aphakia, if both eyes somewhat resemble gullstrand’s emmetropic eye, the retinal image sizes for the two eyes may be essentially the same, but each would be magnified about 28% as compared to the retinal image of the emmetropic eye. When aphakia is corrected by a spectacle lens sometimes enable the aphakic patient to achieve central visual acuity that exceeds the best visual acuity obtained prior to surgery. This single positive outcome of the greatly increased magnification may permit the prescribing of a weaker reading addition than that for the phakic presbyope of the same age, therefore extending the range of vision through the bifocal segment and reducing the convergence demand.
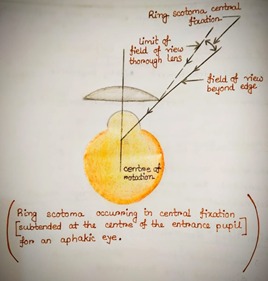
- The base-to-the-center prismatic effect of a high plus lens reduces the size of the field of view through the lens. The aphakic patient suffers more from loss of macular field of view than from loss of peripheral field of view. The loss of peripheral field of view is about 7 degrees whereas the loss of macular field is 17 degrees. This loss of both peripheral and macular field field of view when wearing a high plus lens is responsible for the RING SCOTOMA.
- The presence of ring scotoma is the most disturbance part. There is “ROVING RING SCOTOMA” and the phenomenon occurs is “JACK-IN-THE-BOX” phenomenon. The stronger the lens power the larger the ring scotoma. The farther the lens from the eye, the smaller the ring scotoma. But unfortunately, moving the lens further out makes the ring scotoma move centrally. Therefore, the closer the vertex distance the less bothersome the ring scotoma will be. As lens size increases, the ring scotoma increases in size,but it also moves toward the periphery. The smaller the pupil, the larger the ring scotoma. As lens thickness increases, so does the magnification and the size of the ring scotoma. With increasing steepness of the base curve, both the magnification and the size of the ring scotoma increases.
- When a spectacle lens is worn, the angle the eye must turn in changing fixation from one object point to another increases for high plus lenses in comparison with the angle that would be required without the lens.
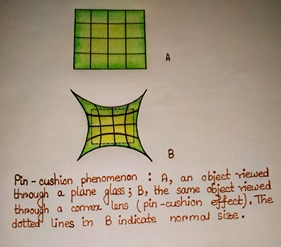
- Spherical aberration due to thick aphakic lenses also pose a problem, producing PIN-CUSHION distortion. The patient finds himself or herself in a parabolic world; i.e. the straight line becomes curve.
- Thick glasses cosmetically embarrassing as the eyes also appear larger behind the glasses.
- The patient may complain of coloured hue in the vision.
- There will be poor depth of vision/stereopsis.
CONTACT LENSES:
- Aphakic contact lense is not very common in practice. It is treatment of choice who is unsuitable for IOL implantation or who have experienced a failed IOL implantation. Contact lense is very common in unilateral aphakia. Contact lense provide less image magnification (about 5-7%) which make possibility of binocular single vision in uniocular aphakia.
- Provide binocular single vision only where fellow eye has useful vision
- Can achieve only 140 seconds of arc (titmus)
- 80% with intermittent suppression
- Provide binocular single vision only where fellow eye has useful vision
- Contact lenses options for aphakia:
- Hydrogel lenses: cases with low astigmatism or failed RGP lens wearer.
- RGP lenses: cases with high corneal astigmatism and corneal distortion.
- Silicon elastomer: cases with low astigmatism and pediatric aphakic patients.
- Sclera lenses: patients with significant corneal distortion.
- Tinted lenses: to attenuate bright light and offer some UV protection.
- Multifocal contact lenses: as per patient condition.
- Bifocal contact lenses: as per patient condition.
- There is some advantages of contact lenses over spectacles :
- Less magnification of image
- Elimination of aberration and prismatic effect of thick glasses
- Wider and better field of vision
- Cosmetically more acceptable
- Better suited for uniocular aphakia
- Disadvantages of contact lenses are :
- More cost
- Cumbersome to wear, especially in old age and in childhood
- Corneal complications may be associated
INTRAOCULAR LENS IMPLANTATION:
- Intraocular lens implantation is the best available method of correcting aphakia.
- Difficult to implant IOL in congenital cataract due to small size of eyeball. IOL power may hamper the emmetropization process due to inappropriate IOL size and power. In unilateral cases, primary implantation is indicated as soon as the patient is fit for anaesthesia, ideally between 2 to 3 months of age. The earlier the surgery is done, the better the chance that deep amblyopia can be overcome.
- Incase of unilateral congenital cataract most studies suggested that surgery after 6 weeks of life is less likely to result good visual acuity.
- In bilateral congenital cataract difference between surgery of two eye must be less than 6 weeks. Bilateral congenital cataract is more common than unilateral cataract. In major blood vessels can not be distinguished from central portion of the cataract significant visual deprivation can be expected from moderately size partial cataract.
Types of IOL:
Manufacturing type:
- Monofocal IOL
- Multifocal IOL
- Toric IOL
- Blue light filtering PIOL
Positional type:
- AC IOL
- Iris fixated PIOL
- Sulcus supported PIOL
- Scleral hooking IOL
Advantages of IOL implantation:
- Little image magnification
- No spherical and prismatic aberration
- Minimum or no aniseikonia
- Normal peripheral field
- Cosmetically well accepted
Disadvantages of IOL implantation:
- Infections
- Expulsive choroidal hemorrhage
- Cystoid macular edema
- Retinal detachment
- Corneal edema
- Dislocation of IOL (child rubbing eye)
- Posterior capsular opacities
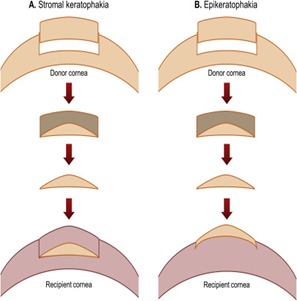
REFRACTIVE CORNEAL SURGERY:
- Refractive corneal surgery is under trial for correction of aphakia. It includes :
- Keratophakia. In this procedure, a lenticular prepared from the donor cornea is placed between the lamellae of the patient’s cornea.
- Epikeratophakia. In this procedure, a lenticule prepared from the donor cornea is stitched over the surface of patient’s cornea after removing the epithelium.
- Hyperopic laser – assisted in situ keratomileusis.








{kind=link}