
PUPIL AND IT’S FUNCTIONS:-
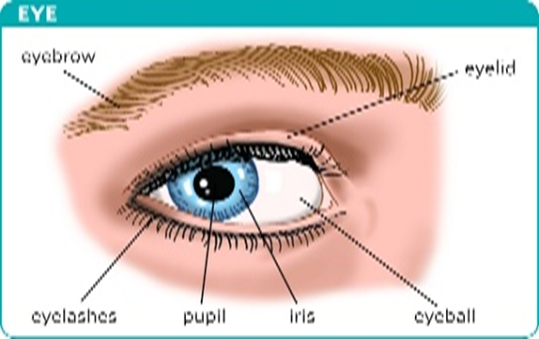
Pupil is the aperture or an entrance in iris through which the light enters in our eye and reach to retina. It is mainly surrounded by sphincter pupillae muscle and dilator pupillae muscle that limits the amount of light to be entered in eye in different situations by constriction (i.e; decreasing the pupillary diameter) or by dilatation (i.e; increasing the pupillary diameter).
Functions of pupil are:-
- Regulating the amount of light to be entered based on retinal adaptation state.
- Helps in increasing the depth of focus, when seeing near objects.
- Also helps in reducing optical aberrations such as e.g. peripheral aberration, chromatic aberration and few amount of astigmatism.
Nerve supply:- The sphincter pupillae muscle is supplied by parasympathetic system through the 3rd cranial nerve (oculomotor nerve) and the dilator pupillae muscle is supplied by the adrenergic fibers of the cervical sympathetic nerve.
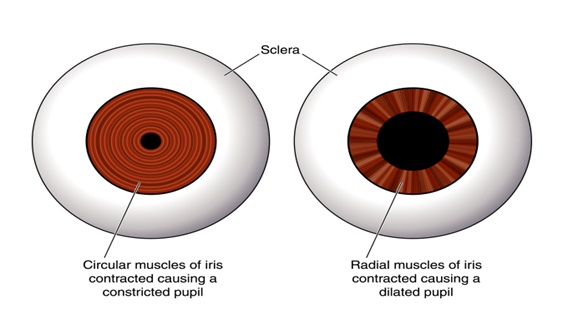
The dilation of pupil occurs due to contraction of dilator pupillae muscle and relaxation of sphincter pupillae muscle.
The constriction of pupil occurs due to contraction of sphincter pupillae muscle and relaxation of dilator pupillae muscle.
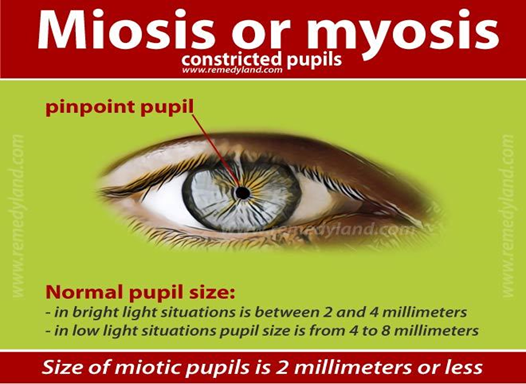
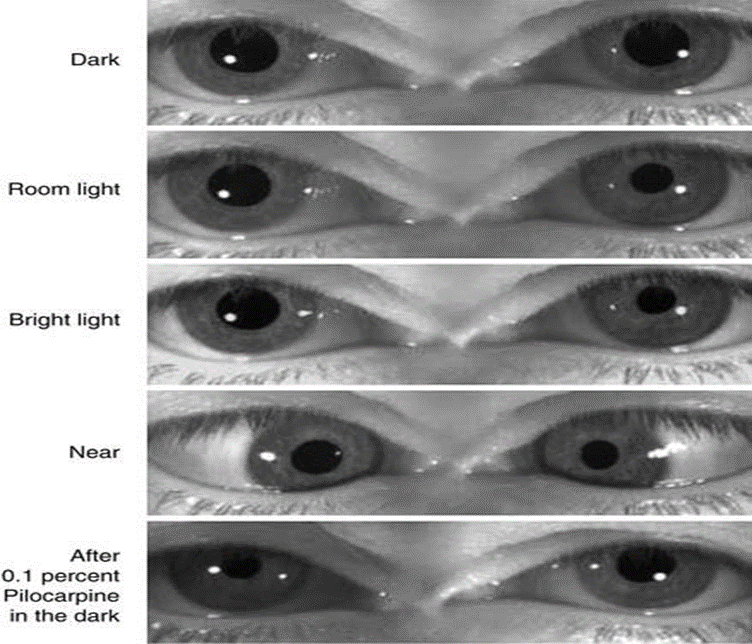
The diameter of pupil can vary from 1mm to 9mm as per the background illumination or actions of muscles. The best retinal image can be found with diameter of 2.8mm and the pupil below 2mm is considered to be mitotic pupil or pinpoint pupil.

PUPILLARY REFLEXES:- There are all total three pupillary reflexes – Light reflex, Near reflex and Psychosensory reflex.
- Light Reflex: When light is shone to either of the eyes both the pupil constrict. The constriction of pupil in which the light is shone is called Direct light reflex and that of the other pupil is Consensual or indirect light reflex. Both reflexes are initiated by retinal photoreceptors that is rod cell and cone cell.
Light reflex pathway:
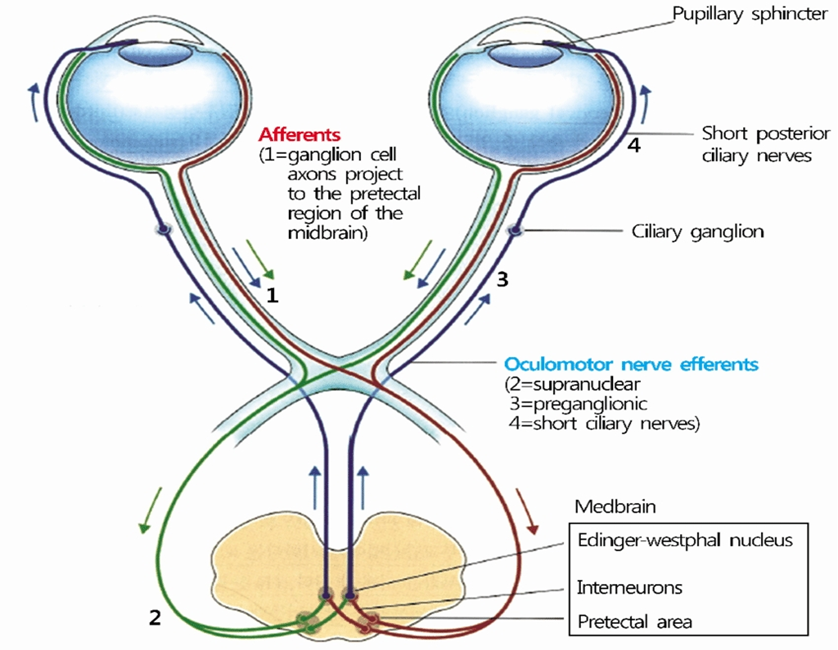
- Afferent fibres are extended in midbrain from retina up to the pretectal nucleus. Then it travel along the optic nerve to the optical chaisma where fivers from the nasal retina of each eye cross and travel along the opposite optic tract to terminate in the contralateral pretectal nucleus. And the fibers from the temporal retina will remain uncrossed and will Continue along the optic tract of the same site to terminate in the ipsilateral pretectal nucleus.
- Internuncial fibres it connects each pretectal nucleus with Edinger-Westphal nuclei from both sides and This connection forms the base of consensual light reflex.
- Efferent pathway it consists of the parasympathetic fibres which arise from the Edinger-Westphal nucleus in the midbrain and travel along the oculomotor nerve. The pre ganglionic fibres enter the inferior division of the third nerve and via the nerve to the inferior oblique reach the ciliary ganglion to relay. Postganglionic fibers travel along the short ciliary nerves to innervate this sphincter pupillae.
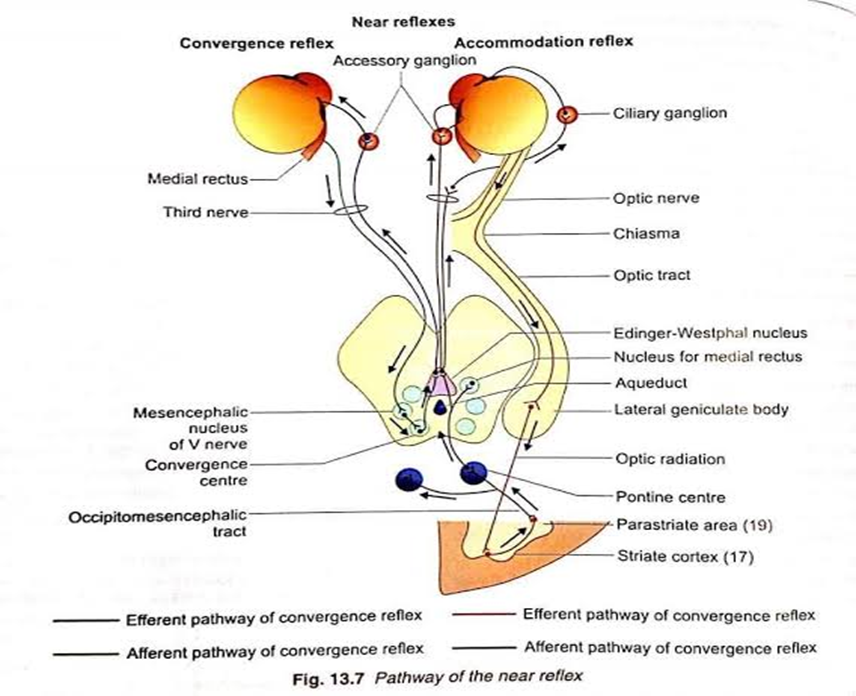
- Near reflex: it occurs when we look at near object. This contains two main components (1) Convergence reflex, i.e., constriction of pupil on convergence and (2) Accommodation reflex, i.e., constriction of pupil along with accommodation.
Convergence reflex pathway: Here afferent pathway is still not cleared. There is a assumption that afferent fibers from the medial rectus travel centrally through the oculomotor nerve to the mesencephalic nucleus of the trigeminal nerve, To a presumptive centre of convergence in the tectal or pretectal region. By this the impulse is relayed to the Edinger-Westphal nucleus and the subsequent efferent pathway of near reflex is along the oculomotor nerve. This efferent fibres relay in the accessory ganglion before reaching the sphincter pupillae muscle.
Accommodation reflex pathway: Here afferent impulses are extended from the retina to the parastriate cortex through the “optic nerve, optic chiasma, optic tract, lateral geniculate body, optic radiations and striate cortex. From the parastriate cortex, the impulses are relayed to the Edinger-Westphal nucleus of both sides through the occipitomesencephalic tract and the pontine centre. From the Edinger-Westphal nucleus efferent impulses travel with the oculomotor nerve and reach the sphincter pupillae muscle and ciliary muscle after relaying in the accessory and ciliary ganglion.
- Psychosensory reflex: this basically means the dilatation of the pupil in response to sensory and psychic stimuli and it is very complex and its mechanism is still not cleared.
ABNORMALITIES OF PUPILLARY REFLEXES:-
- Afferent pupillary defect: Also known amaurotic pupil, Refers to a condition in which both the consensual and direct light reflex will be absent When light is shone in the affected eye. It occurs due to a lesion present in optic nerve and it may cause complete blindness of affected eye. The light reflex and near reflex will be present for the normal eye.
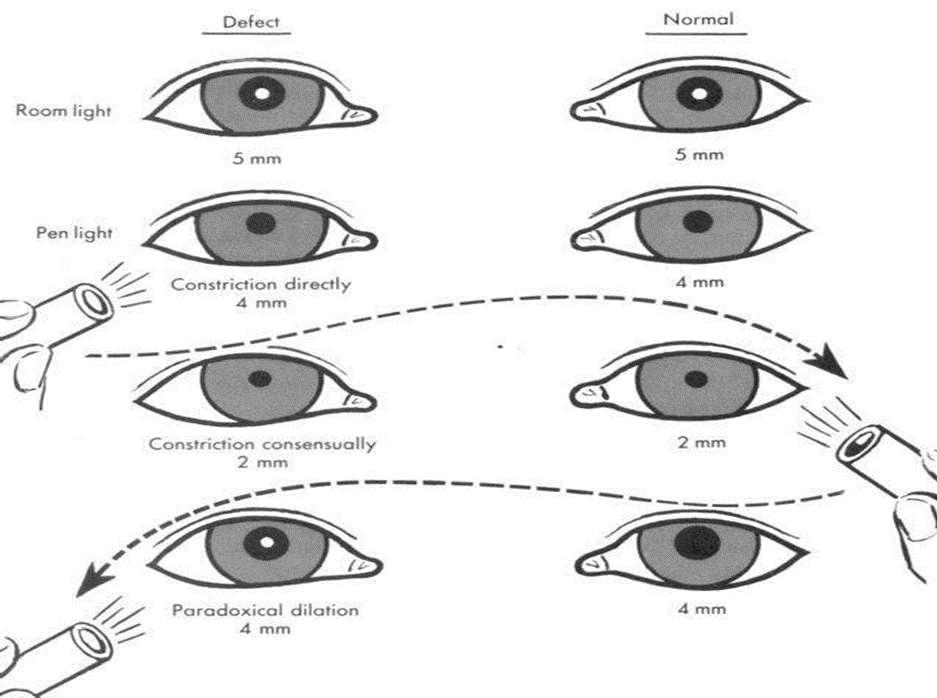
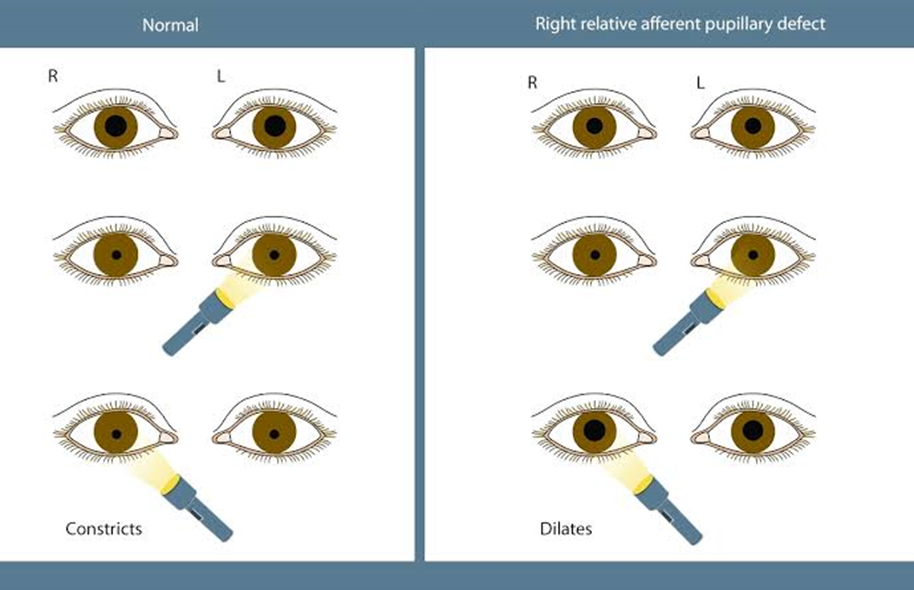
- Relative afferent pupillary defect: Also known as Marcus Gunn pupil. Here the near reflex will be present for both the eyes. When light is shone to the unaffected eye, both consensual and direct reflex will be present and when it will be shone to affected eye both the pupil will dilate. It can easily be detected with swing flash test. It mainly caused by incomplete optic nerve lesion or very severe retinal disease.
- Hippus: Basically it is the alternative rhythmic dilatation and constriction of the pupil and this oscillation are very large and sometimes often independent of the light. It is found in multiple sclerosis.
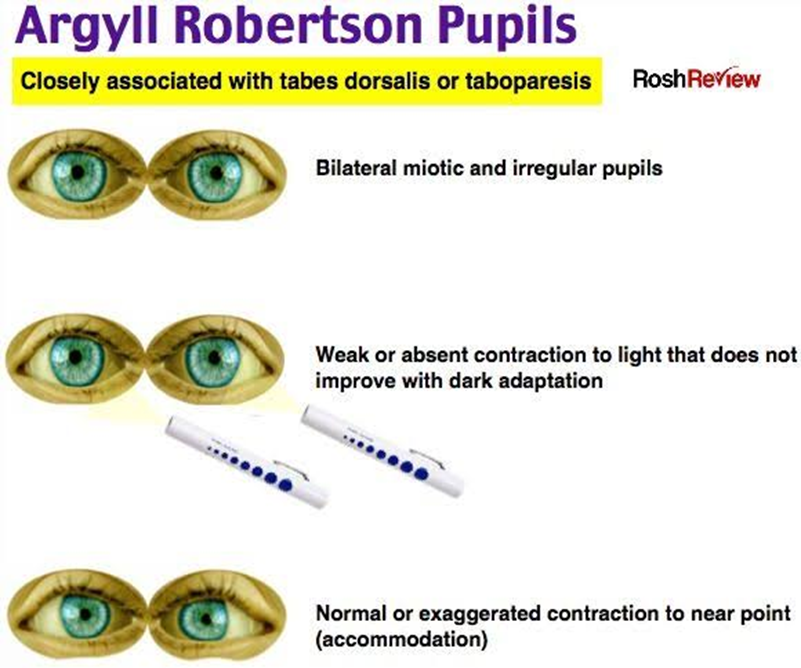
- Argyll Robertson pupil: It is considered to be a bilateral anomaly where the light reflex is absent but the near accommodation reflex is present. Pupils are slightly miotic irregular e centric and unequal. Most of the time people fails to dilate with mydriatics but constricts with mitotics. It mainly caused due to the lesions of neurosyphilis in the region of pre tectum.
Adie’s tonic pupil: Basically it is idiopathic but it is believed to be caused by post ganglionic parasympathetic pupillomotor damage. Here the affected eye is always larger that is having anisocoria and the light reactions and near reactions for affected i will be and the light reactions and near reactions for affected eye will be sluggish.








{kind=link}