
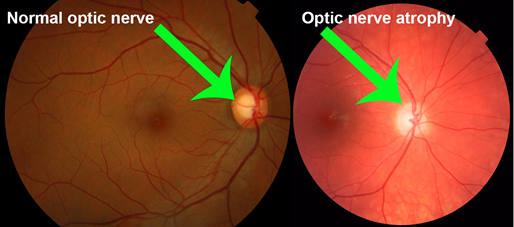
Optic atrophy refers to the late stage changes that take place in the optic nerve resulting from axonal degeneration in the pathway between the retina and the lateral geniculate body, manifesting with disturbance in visual function and in the appearance of the optic nerve head.
Frequency
Optic atrophy type 1 is estimated to affect 1 in 35,000 people worldwide. This condition is more common in Denmark, where it affects approximately 1 in 10,000 people.
Causes
What causes optic atrophy?
The optic nerve is composed of nerve fibers that transmit impulses to the brain. In the case of optic atrophy, something is interfering with the optic nerve’s ability to transmit these impulses. The interference can be caused by numerous factors, including:
Glaucoma.
Stroke of the optic nerve, known as anterior ischemic optic neuropathy.
A tumor that is pressing on the optic nerve.
Optic neuritis, an inflammation (swelling) of the optic nerve caused by multiple sclerosis.
A hereditary condition in which the person experiences loss of vision first in one eye, and then in the other (known as Leber’s hereditary optic neuropathy).
Improper formation of the optic nerve, which is a congenital problem (the person is born with it)
General Pathology
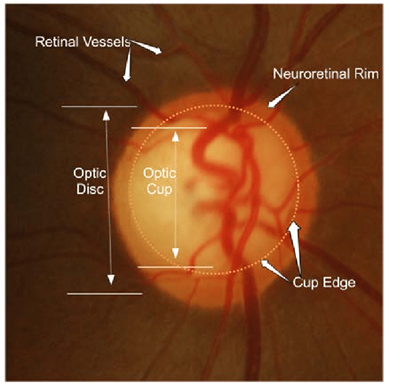
The optic nerve is a bundle of 1.2 million axons of retinal ganglion cells that carries visual information from the retina to the brain. The optic nerve is myelinated by oligodendrocytes that do not regenerate after damage. In optic nerve atrophy there is loss of axons and shrinkage of myelin leading to gliosis and widening of the optic cup.
Types
Primary optic atrophy
Primary optic atrophy occurs without antecedent swelling of the optic nerve head. It may be caused by lesions affecting the visual pathways at any point from the retrolaminar portion of the optic nerve to the lateral geniculate body. Lesions anterior
to the optic chiasm result in unilateral optic atrophy, whereas those involving the chiasm and optic tract will cause bilateral chsnges.
Signs
○ Flat white disc with clearly delineated margins.
○ Reduction in the number of small blood vessels on the disc surface.
○ Attenuation of peripapillary blood vessels and thinning of the retinal nerve fibre layer (RNFL).
○ The atrophy may be diffuse or sectoral depending on the cause and level of the lesion. Temporal pallor of the optic nerve head may indicate atrophy of fibres of the papillomacular bundle and is classically seen following demyelinating optic neuritis. Band atrophy is a similar phenomenon caused by involvement of the fibres entering the optic disc nasally and temporally. It occurs in lesions of the optic chiasm or tract and gives nasal as well as temporal pallor.
• Important causes
○ Optic neuritis.
○ Compression by tumours and aneurysms.
○ Hereditary optic neuropathies.
○ Toxic and nutritional optic neuropathy, which may give temporal pallor, particularly in early/milder cases when the papillomacular fibres are preferentially affected
○ Trauma.
Secondary optic atrophy
Secondary optic atrophy is preceded by longstanding swelling of the optic nerve head.
• Signs vary according to the cause and its course.
Slightly or moderately raised white or greyish disc with poorly delineated margins due to gliosis
○ Obscuration of the lamina cribrosa.
○ Reduction in the number of small blood vessels on the disc surface..
○ Peripapillary circumferential retinochoroidal folds, especially temporal to the disc sheathing of arterioles and venous tortuosity may be present
.
• Causes include chronic papilloedema, anterior ischaemic optic neuropathy and papillitis. Intraocular inflammatory causes of marked disc swelling are sometimes considered to cause secondary rather than consecutive atrophy
Consecutive optic atrophy
Consecutive optic atrophy is caused by disease of the inner retina or its blood supply. The cause is usually obvious on fundus examination, e.g. extensive retinal photocoagulation, retinitis pigmentosa or prior central retinal artery occlusion. The disc appears waxy, with reasonably preserved architecture
Symptoms
The main symptom of optic atrophy is vision loss. Any other symptoms are attributable to the underlying process that caused the disc damage (such as pain with angle closure glaucoma).
Physical diagnosis
A complete eye exam including visual field, assessing color and contrast vision, intraocular pressures, looking for afferent pupil defect, and fundoscopy should be done
Treatment
Pharmacological treatment for optic atrophy has been largely ineffective. The only focus in management in treating the exact cause before the development of significant damage to slavage useful vision.
Once the condition is stabilized low vision aids cab be prescribed to individuals.
Pulse intravenous methylprednisolone has been be used in condition such as optic neuritis, artertic anterior ischemic optic neuropathy and traumatic optic neuropathy.
Stem cell treatment may prove to be key in future treatment of neuronal disorders. Neural progenitor cells can be delivered to the vitreous from where they can intergrate into ganglion cell layer of retina.
These cells would turn on neurofilament genss, and migrated into the host optic nerve to stimate the regeneration of neural elements.







{kind=link}