
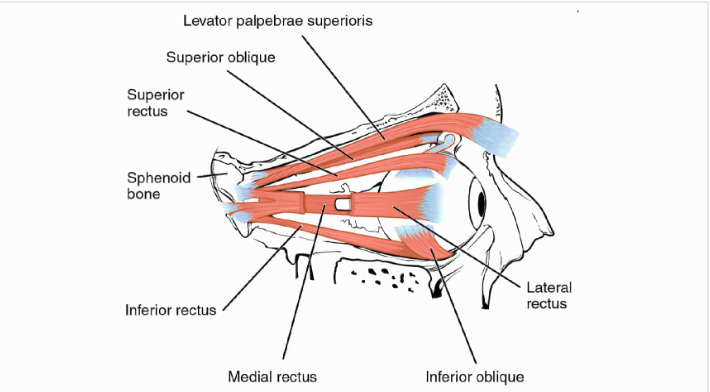
The extraocular muscles are a group of six muscles located around the eye, working in
perfect harmony to control its movement. These muscles are named based on their location
and primary function. Let’s meet these unsung heroes:
Medial Rectus (MR)
Course: The medial rectus originates from the medial part of the annulus of Zinn at the
orbital apex and passes forward to get inserted at around 5.5mm away from the limbus. The
medial rectus has the shortest tendon (4.5mm) among all the recti muscles. This is the only
rectus muscle with no oblique muscle running tangentially.
Action – Adduction
Innervation – Oculomotor nerve (Third cranial nerve)
Lateral Rectus (LR)
Course: The lateral rectus originates from the lateral part of the annulus of Zinn and
progresses forwards to get inserted approximately 6.9mm from the limbus. The lateral
rectus muscle has the broadest arc of contact, i.e., 12mm, among all the recti muscles. The
lateral rectus is the thinnest extraocular muscle having a width of only 9.2 mm. The
intermuscular septa attach the lateral rectus to the inferior oblique muscle.
Action – Abduction
Innervation – Abducens nerve (Sixth cranial nerve)
Superior Rectus
Course: The superior rectus muscle originates from the superior part of the annulus of Zinn
and proceeds anteriorly along the orbital wall to get inserted into the sclera at a distance of
approximately 7.7mm from the limbus. The superior rectus is attached to the fibres of the
levator palpebrae superioris that courses above this muscle from the point of origin. The
superior oblique muscle lies between the superior rectus and the sclera. Both the muscles
are connected to each other by the intermuscular septa.
Action– Primary action is elevation. Additional actions include incyclotorsion and adduction.
Innervation– Oculomotor nerve (Third cranial nerve)
Inferior Rectus
Course: The inferior rectus muscle originated from the inferior part of the annulus of Zinn
and then proceeds anteriorly to get inserted at an approximate distance of 6.5mm from the
limbus. The inferior oblique muscle passes beneath the inferior rectus. The inferior rectus
muscle is also strongly connected to the lower eyelid retractors.
Action– Primary action is depression. Additional actions include excyclotorsion and
adduction.
Innervation– Oculomotor nerve (Third cranial nerve)
Superior oblique
Course: The superior oblique muscle originates from the periosteum of the sphenoid bone,
superomedial to the optic foramen, and the common tendinous ring. It then progresses
anteriorly, parallel to the medial wall of the orbit, to reach the trochlea. Trochlea is a
cartilaginous loop attached to the frontal bone's nasal part. After looping from the trochlea,
the muscle becomes a tendon, turning posterolateral and passing beneath the superior
rectus. It finally gets inserted posterior and lateral to the insertion of the superior rectus, as
shown in Figure 4. The superior oblique is the longest muscle of all the extraocular muscles.
Action– Primary action is incyclotorsion. Additional actions include depression and
abduction.
Innervation– Trochlear nerve (Fourth cranial nerve)
Inferior Oblique
Course: It originates from the orbital floor lateral to the nasolacrimal groove. The muscle
then runs along the orbit floor and crosses below the inferior rectus muscle. It then ascends
posterolateral to pass between the lateral rectus and the orbit floor. It then inserts posterior
to the equator in the inferolateral quadrant onto the sclera. The fascial sheath of the
inferior oblique blends with the sheath of the inferior rectus, which then blends with the
medial and lateral check ligaments. The fusion of all these forms the suspensory ligament of
the eyeball, which is a hammock-like sling that supports the eyeball. The inferior check
ligament is an anterior expansion from the fused sheaths of the inferior rectus and oblique
muscles that attach to the tarsus muscle of the lower eyelid.
Action– Primary action is excyclotorsion. Additional actions include elevation and abduction.
Innervation– Oculomotor nerve (Third cranial nerve)
Levator Palpebrae Superioris (LPS)
Course: The LPS is a thin triangular muscle extending along the bony orbit’s roof. It
originates from the inferior aspect of the lesser wing of the sphenoid, superior to the
annulus of Zinn. The muscle originates as a short and narrow tendon, which fans out and
gradually widens as it courses anteriorly. Once it reaches the Whitnall’s ligament, a
transverse suspensory ligament, the LPS muscle becomes more tendinous and changes its
direction to become vertical, called the vertical levator aponeurosis. The levator
aponeurosis has multiple insertions. The aponeurosis has medial and lateral wings which
attach to the medial and lateral canthal tendons, respectively. It inserts anteriorly into the
upper eyelid skin, inferiorly into the anterior surface of the upper tarsal plate, and has few
extensions to the superior conjunctival fornix.
Action- Elevates upper eyelid
Innervation- Oculomotor nerve (Third cranial nerve)
Nerve Supply – The Lifeline of Eye Movements
Now that we've met our stellar cast of extraocular muscles, it's time to learn about their
nerve supply. The oculomotor nerve (cranial nerve III) controls four of the six muscles
(superior rectus, inferior rectus, medial rectus, and inferior oblique). The trochlear nerve
(cranial nerve IV) innervates the superior oblique, and the abducens nerve (cranial nerve VI)
controls the lateral rectus. This precise innervation ensures the eyes work harmoniously to
track moving objects and maintain binocular vision.
Clinical Perspectives – When Harmony Is Disrupted
Despite their incredible coordination, extraocular muscles can face challenges. Strabismus,
commonly known as crossed eyes, occurs when there is a misalignment of the eyes due to
an imbalance in muscle function. Disorders affecting the cranial nerves can also lead to
impaired eye movements.








{kind=link}