
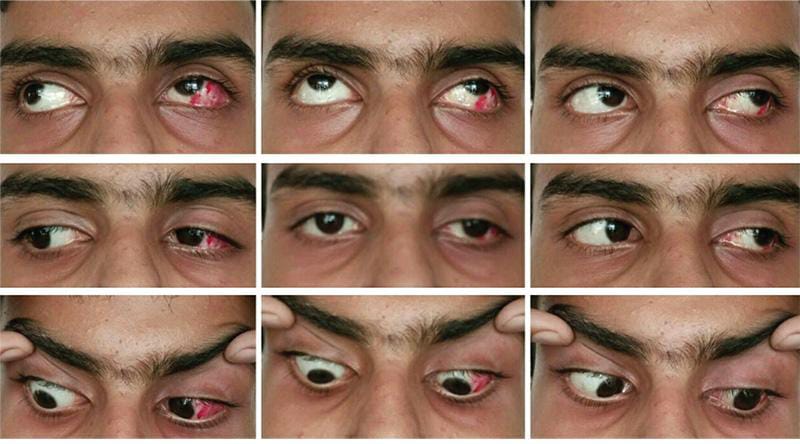
- INTRODUCTION:-
Exodeviation that develops iatrogenically after esotropia surgery is called consecutive exotropia. This deviation occurs according to Von Noorden between 2% – 8%. While other studies found an incidence ranged from 4% to 27%. This surgical complication can develop immediately after surgery or many years and even decades later, some risk factors causing its development have been reported by ophthalmologist like high hyperopia, amblyopia, vertical deviation, A and V patterns, nystagmus, large medial rectus recessions, restriction of adduction, multiple surgeries, and developmental delay, the failure to evaluate the patient condition preoperatively.
The surgical treatment of this category of strabismus encloses more options on horizontal rectus muscles that are differently used by different authors. Some authors recommend to perform surgeries on muscles which have been already operated in order to avoid manipulation of intact muscles. On the contrary, some surgeons assume that surgery on previously operated muscles is unpredictable and recommend recession of the LR muscles.
But, all authors accept that the decision regarding the surgical procedure to be taken involves an assessment of the type and amount of previous surgery and the presence of limitation of adduction (sometimes to the presence of scar traction) or convergence insufficiency. It was established that, large recessions, exceeding 5 mm of the MRM can produce consecutive exotropia associated with limitation of adduction; large resections of the lateral rectus muscle can cause in contrary a limitation of abduction. Usually recession is indicated for patients with consecutive exotropia with limited adduction after bilateral MRM recession, or in cases that underwent unilateral MRM recession/LRM resection surgery. For patients with divergence excess or exotropia with normal MRM function a bilateral LRM recession is indicated, but it should be avoided in patients with limitation of adduction. But one thing is actual concerning consecutive exotropia—it requires special attention of the orthoptist and surgeons, due to the difficulties in pre-operative assessment, in planning and even performing the surgery.
- WHY CONSECUTIVE EXOTROPIA OCCURS:-
- Usually after esotropia surgery.
- The esotropia correction doesn’t ‘grow’ with the patient,
- Perfect early alignment after congenital esotropia surgery – 30% consecutive exotropia after 25years of age.
- Recession MR:- mechanical disadvantage.
- EARLY CONSECUTIVE EXOTROPIA:- due to,
- Wrong surgical dose.
- Poor surgical technique.
- Poor early healing.
- LATER CONSECUTIVE EXOTROPIA:- due to,
- Stretched scar- look for stretchmarks healing of other surgical scars.
- Irene Ludwig- scar remodeling & scar migration.
- Scar remodeling after strabismus surgery- very under recognized,
- Need to use absorbable sutures if recognized.
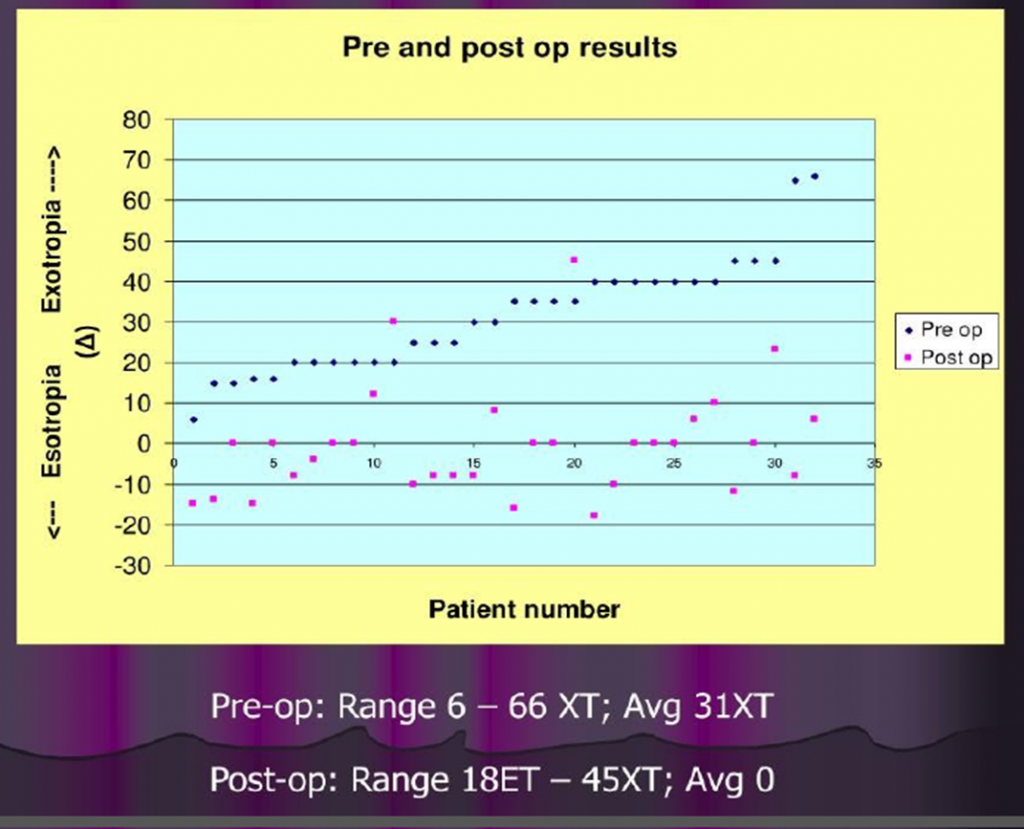
PRE & POST OPERATIVE RESULTS :-
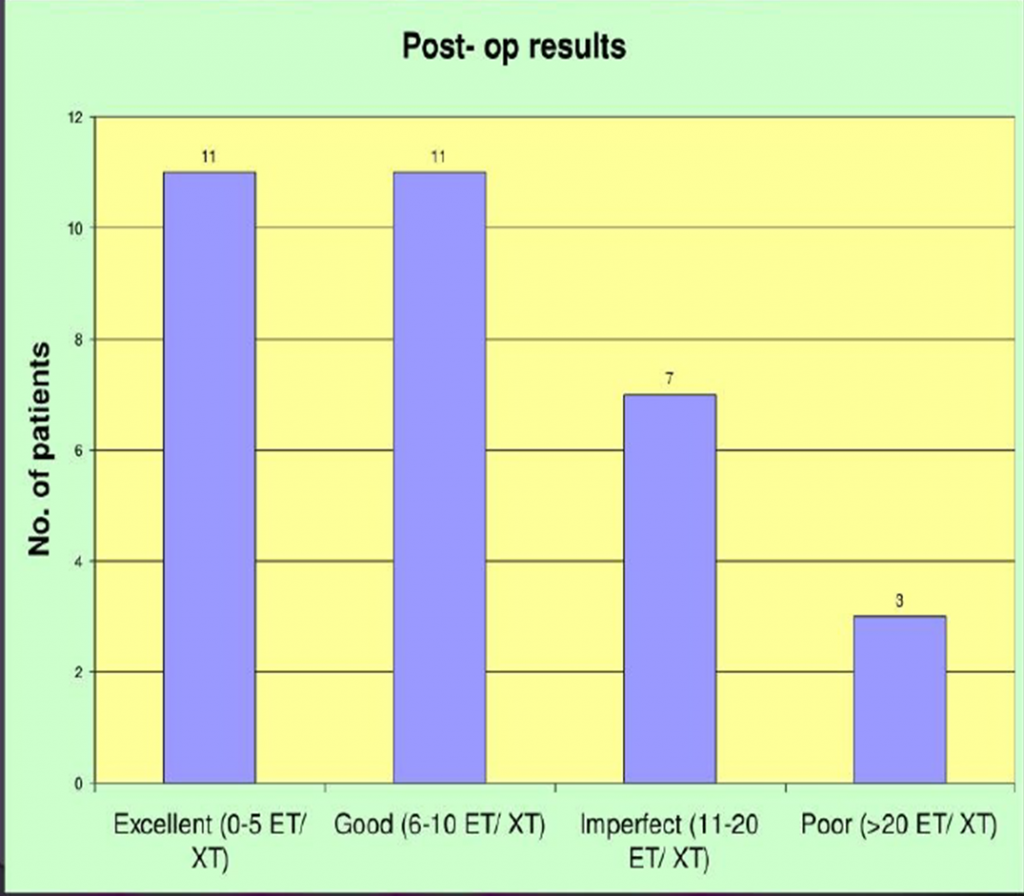
POST OPERATIVE RESULTS :-
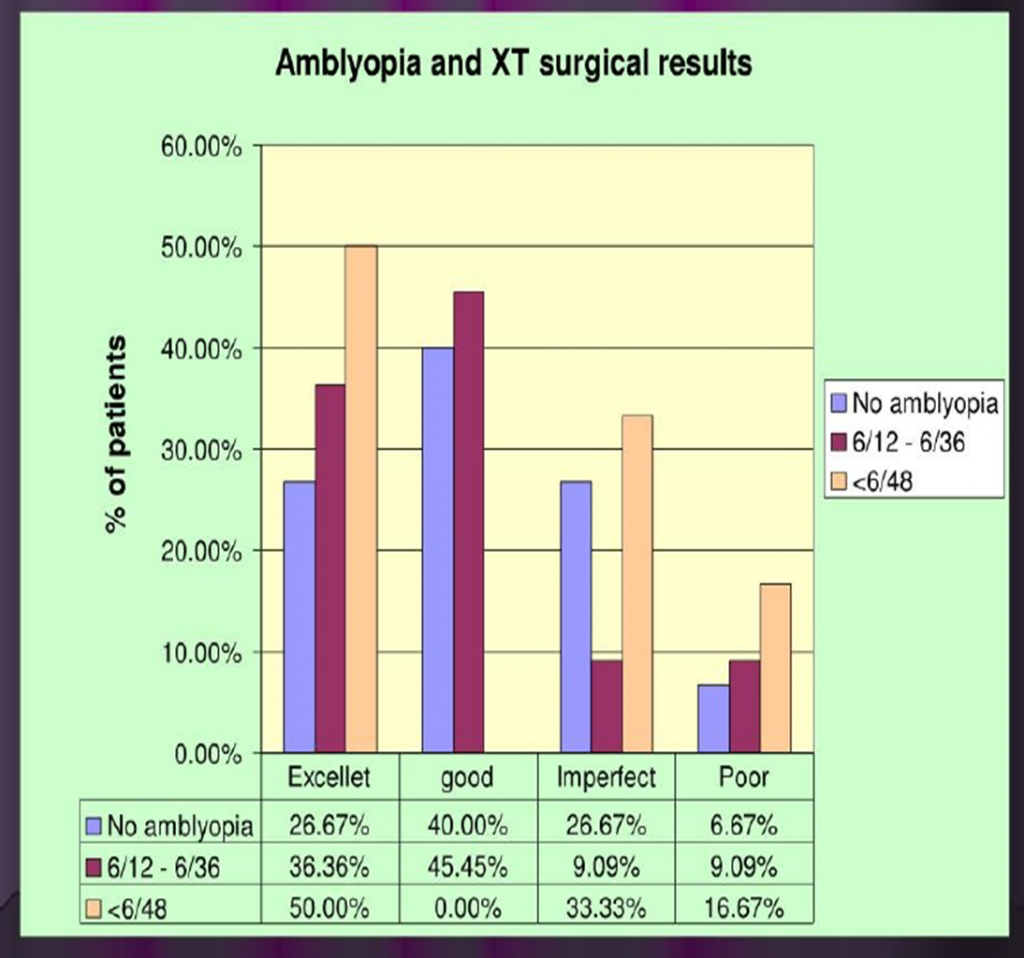
AMBLYOPIA & EXOTROPIA SURGICAL RESULTS:-
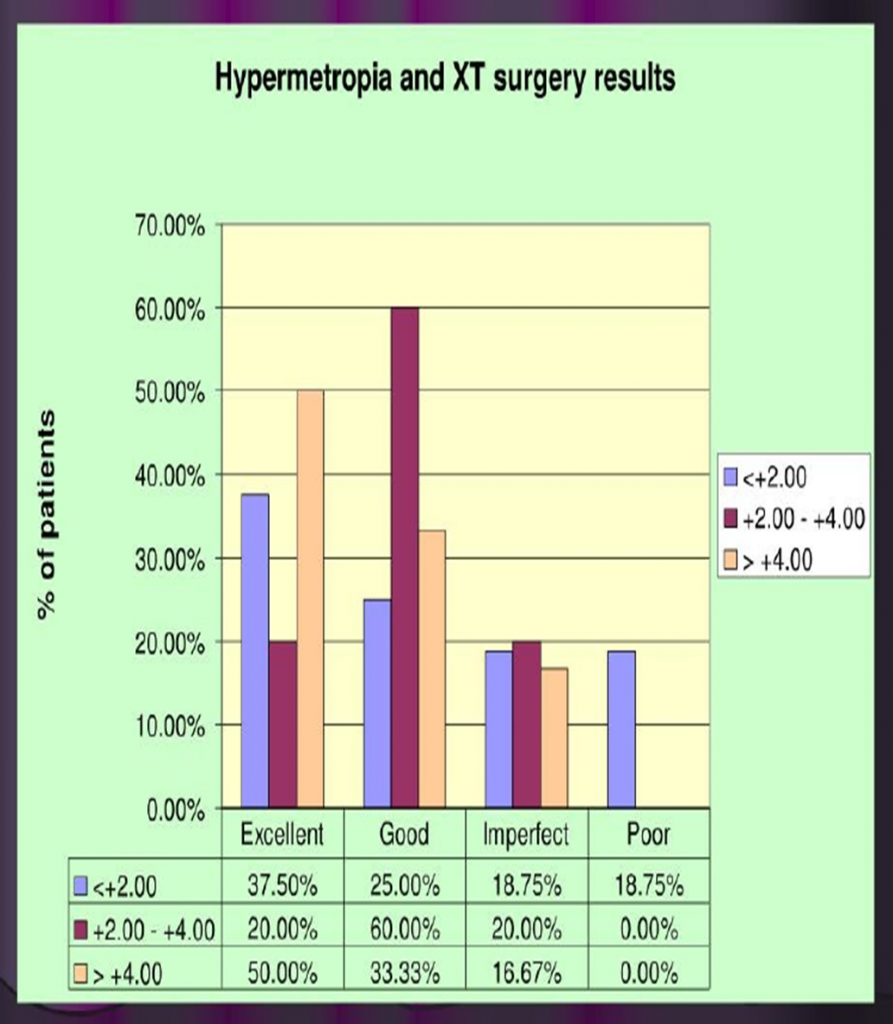
HYPEROPIA & EXOTROPIA SURGERY RESULTS :-
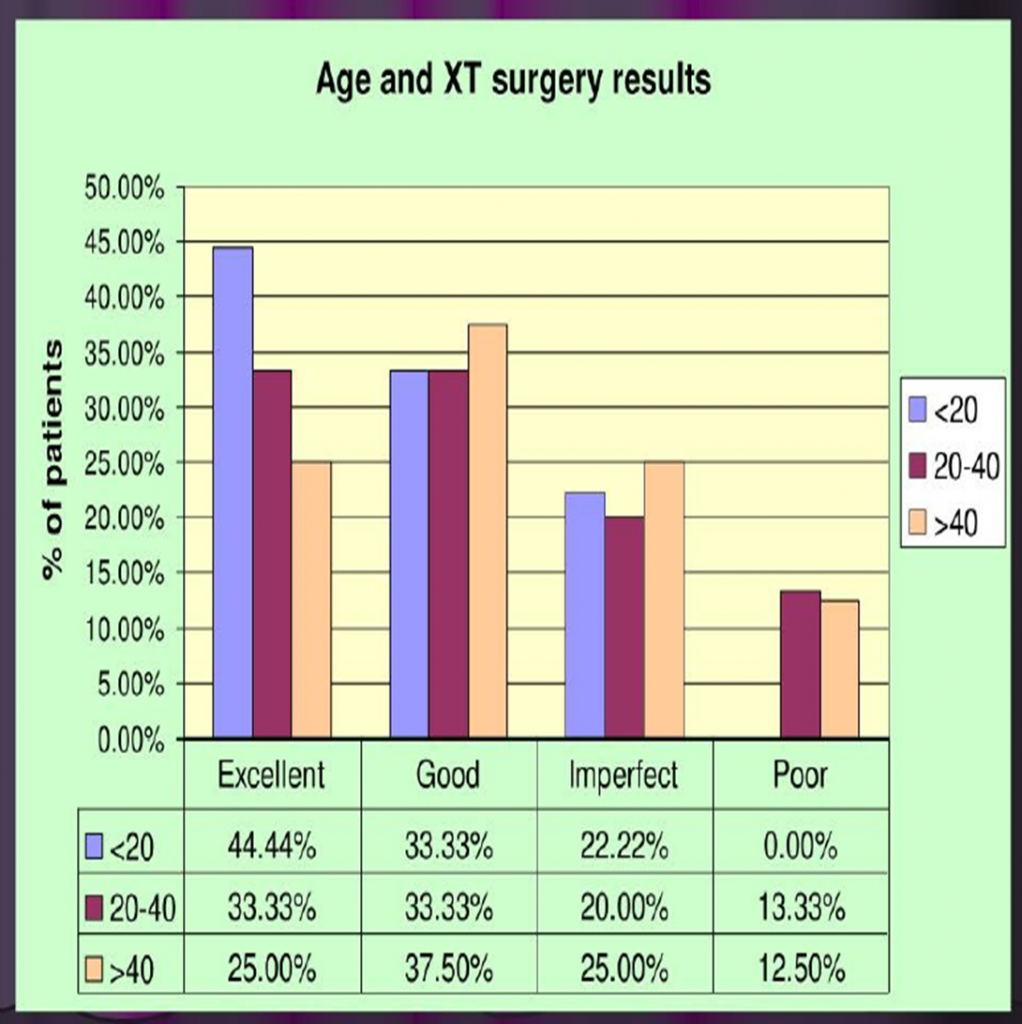
AGE & EXOTROPIA SURGERY RESULTS:-
SURGICAL MANAGEMENT OF CONSECUTIVE EXOTROPIA:- (long term outcomes)
- PURPOSE:- To compare lateral rectus recession(LRc) & medial rectus advancement (MRadv) for correction of consecutive exotropia.
- METHODS:– Of the 43 exotropia pt. 20 of them underwent LRc (group A) & 23 of them underwent MRadv(group B).
- RESULTS:- An avg. dose effect in group B is higher than group A in the early postoperative period, however there was no significant difference at the second year of follow-up. An avg. exodrift after 2year follow-up was 6,6 plus minus 7, 12 PD in group A & 8,13 plus minus 7,45PD in group B. Postoperative overall success rate was 50% in group A & 65% in group B.
- DISCUSSION:- Consecutive exotropias are manifest exotropias that occurfollowing surgery for esotropia. Consecutive exotropias are much more common than consecutive esotropias. Most of the previous studies have shown time duration of 8.7-30 years between surgeries for esotropia to exotropia. Risk factors include adduction deficit, amblyopia, anisometropia, A or V pattern, dissociated vertical deviation (DVD), hypermetropia, absent or poor binocularity and iatrogenic causes (ie, previous medial rectus recession of >7 mm, multiple surgeries, miscalculation). In a study of 20 patients with consecutive exotropia, medial rectus slippage was found to be present in about 1/3 of patients. In this study, medial rectus advancement effectively treated consecutive exotropia without regard to muscle slippage. Most of the previous studies have advocated medial rectus advancement as the first step for consecutive exotropia in the presence of preoperative adduction deficit. These studies have shown dose effect relationship of medial rectus advancement for consecutive exotropia as 3-5 PD/mm. However, Mohan et al9 advocated unilateral lateral rectus recession and medial rectus resection and they found no significant advantage of adding medial rectus advancement. Muscle slippage is a common cause of consecutive exotropia. Muscle slippage may occur immediately with limited ductions after strabismus surgery, but it may also occur progressively. Signs of acute medial rectus muscle slippage include a large exotropia associated with limited adduction and palpebral fissure widening on adduction. Detection of acute muscle slippage is not difficult. However, delayed medial rectus slippage, thought to be more common, may not be as easily recognized. Ludwig and Chow attributed this to stretched scar, an amorphous connective tissue interposed between an operated muscle tendon and sclera that presents with minimal or no version limitation, less separation of the tendons from the sclera, and thicker appearance of the scar segments. Management of consecutive exotropia is challenged by occurrence of late exodrift. Considering this late post operative exodrift, some authors have suggested to aim for overcorrection of 10-15 PD in visually mature patients. Thus, to conclude, medial rectus advancement is preferred in the first stage for consecutive exotropia because it allows surgical exploration of the medial rectus muscle to detect the presence of an unfavorable insertion. Postoperative exodrift should be considered when determining the target angles for consecutive exotropia surgery. Although medial rectus advancement reliably corrected exotropia in the immediate postoperative period, patients should be counseled that eventual recurrence of exotropia is likely.








{kind=link}