
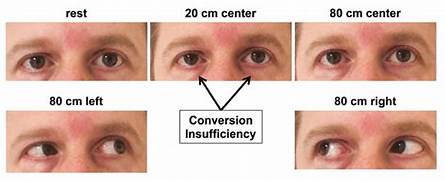
Introduction– Inability to obtain and/or maintain adequate binocular convergence for any length of time without undue effort.
Etiology– 1. Primary or idiopathic — In many cases, exact atiology of convergence insufficiency is not known. It may be associated with a wide IPD and delayed or inadequate functional development. General debility, Psychological instability, overwork and worry maybe the precipitating factors.
2. Refractive errors–convergence insufficiency may be associated with uncorrected high hypermetropia and myopia. Diseases of accommodation convergence mechanism resultin convergence insufficiency in such patients as follows.
*High hypermetropes — usually make no effort to accommodate and thus there is deficient accommodative convergence as well.
* myopes — may not need accommodation and thus lack accommodative convergence. *full convex spherical correction.
3. Presbyopia –with advent of presbyopia, the near point of eye recedes and so there is less use of convergence. Neglect of presbyopia may lead to fixation of this anomaly. on the other hand, patients may also develop convergence insufficiency with the first time use of presbyopic correction. This has been explained by the fact the the relief of sustained accommodation effort afforded by the use of presbyopic correction causes a decrease of accommodative convergence.
4. muscle im blances — Extraocular muscular imbalances in the form of exophoria, intermittent exotropia and vertical muscle imbalances, if neglected for a long time, maybe associated with convergence insufficiency.
5.consecutive convergence insufficiency–may occur following either recession of medial recti or resection of lateral recti muscles.
6. others factors — wide IPD, Delayed or inadequate functional development, general debility over work.
clinical features—1. More in desk workers.2. Asthenopia.3. Not satisfied with glasses.4. Blurred near vision.5. Intermittent crassed diplopia.
Diagnosis—1. Near point convergence >10 Cm.2. Difficulty in attaining 30° of convergence on synoptophore.3. Prism convergence is low but prism divergence is normal.4. Rule out combined accommodation insufficiency and convergence insufficiency.
Differential diagnosis —1. convergence paralysis — there is total lack of ability to overcome any amount of BO prism, whereas in convergence amplitude can be demonstrated. a patient with convergence paralysis will show pupillary constriction but inability to converge, in a patient with convergence insufficiency, pupillary consteriction will occur while converging on an approaching target, followed by dilation of the pupil when convergence can no longer be maintained.
2. Accommodation effort syndrome — usually an exophoria at near is associated with convergence insufficiency, while patients with accommodative effort syndrome have esophoria. convergence insufficiency is helped by the – 3D test, which compensates for the lack of good fasional convergence, whereas a patient with accommodative effort syndrome breaks into a tropia during this test. plus lenses will worsen the convergence insufficiency due to relaxation of accommodative convergence, while they will improve the symptoms in the accommodative effort syndrome for the same reason.
Treatment– convergence insufficiency has an excellent prognosis in the majority of cases. children are treated when fusional vergences doe poor and the patient is showing sings of becoming exotropia. Adults with this condition receive treatment only in the presence of symptoms. Treatment of convergence insufficiency includes optical treatment, or thoptie treatment prism therapy and surgery.1. Excellent prognosis.2. Children treat when fusional vergence is poor and showing sings of exotropia.3. Adults treat when symptomatic
optical treatment–> Myopics should be given full correction.> Hypermetropia should be given under correction. orthoptic treatment–> Exercises to improve near point convergence. *.Advancement exercise.*.jump convergence exercise.> Exercises to increase amplitude of fusional convergence.*.convergence exercise with prisms.*.Exercise using synaptophore.*.convergence card.*.physiologic Diplopia exercise using Stereogram.*.EXercise using Diploscope.
voluntary convergence training—*.proper understanding of procedure and cooperation is needed.*.Explain physiological diplopia.*.Maintain Physiological diplopia for as long as passible and bring in the finger as soon as diplopia is lost.
Relaxation exercise—> Physiologic diplopia with Stereogram in uncrossed position.> Divergence using synoptophore.> Divergence using prisms.
prism therapy–use base-in-prisms for this therapy.
Surgical treatment —Medial rectus muscle resection can be performed in one or both eyes.







{kind=link}