
Accommodation:
Accommodation of the eye is the faculty by which the dioptric power of the eye is changed to be able to focus the objects varying distances. Two objects cannot be in focus at one and the same time. If the distant object is in focus the objects at a nearer or greater distance are out of focus.
This is generally true but even in the absence of accommodative power and if the object is focused at a particular distance it remains in focus while the object is moved closer to or further away from the eye.
At rest, the radius of curvature of the anterior surface of the lens is 10mm and that of the posterior surface is 6mm.
In accommodation, the curvature of the posterior surface remains almost the same, but the anterior surface changes, so that in strong accommodation, its radius of curvature becomes 6mm. The refraction of the eye in this condition is called it’s dynamic refraction.
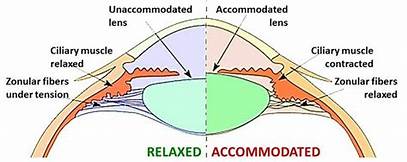
Mechanism of accommodation:
When the eye is at rest and not accommodating the lens is compressed on the capsule by stretched zonule. When the ciliary muscle contracts the choroid is pulled forwards and the ring formed by the ciliary process is narrowed mostly by the circular fibers of the ciliary muscle which now release the tension on the zonule and make it lax. With the relaxation of the zonule the anterior capsule of the lens is also relaxed. The lens has plasticity and, therefore, it moulds itself. The posterior pole rests on the vitreous and cannot mould itself. The moulding occurs in the anterior pole and is determined by the thickness of the capsule. The anterior pole lies opposite the thinnest part of the anterior capsule. In the Pupillary area there occurs a nipple like bulging of the anterior pole of the lens. The lens becomes more spherical. These increase the dioptric power of the eye and thus focus the near object on the retina. During accommodation beside the changes in the lens there is contraction of pupil. The mechanism of accommodation is mediated through a definite nervous pathway. The afferent pathway follows the visual fibers to the striate area of the calcarine cortex and is relayed to the parastriate area. The efferent travel to perlias nucleus via occipital mesencephalic tract. From perlias nucleus fibers go to edinger westphal nucleus from where they are carried to the sphincter through the 3rd nerve via an accessory ganglion.
Range of accommodation:
The distance between the near point and the far point is called the range of accommodation.
•Far point( punctum remotum) is the farthest point at which object can be focused on the retina with ciliary muscle relaxed, and it varies with the emmetropic myopia or hypermetropia.
• near point (punctum proximum) is the nearest point at which small objects can be seen clearly after full accommodation.
[Picture 2]
Amplitude of accommodation:
The difference between the dioptric power needed to focus at near point (P) and far point(R) is called amplitude of accommodation (A). Thus A= P-R.
Amplitude of accommodation and thus the near point of vision (punctum proximum) vary with age.
Physical and physiological accommodation:
•Physical accommodation:- the ability of the lens to alter its shape and it is measured in diopter.
• physiological accommodation:- the power of the ciliary muscle to contract.
The physiological accommodation is the cause, and the physical accommodation is the effect.
There are two other phenomena which occur with accommodation (1) pupils become smaller and (2) convergence of the eyes. Age changes:- as the age advance the amplitude of accommodation progressively decreases from 14D at the age of 10, to 4D at 45years, and by 60 years it is only 1D years near point then being one meter away. This is due to a progressive sclerosis of the lens so that it becomes less malleable, tending to set in unaccommodative shape.
Anomalies of accommodation:
Anomalies of accommodation are not uncommon these include: presbyopia, insufficiency of accommodation, paralysis of accommodation, spasm of accommodation.
Presbyopia:
It means the eye sight of old age. This is a physiological aging process, in which the near point gradually recedes beyond the normal reading or working distance.
Pathophysiology:- to understand the pathophysiology of presbyopia a working knowledge about accommodation is mandatory. As we know, in an emmetropic eye far point is infinity and the near point varies with age being about 7cm at the age of 10years , 25cm at the age of 40 years and 33cm at the age of 45 years. Therefore, at the age of 10 years, amplitude of accommodation (A) = 100/7(dioptric power needed to see clearly at near point) -1/infinite (dioptric power needed to see clearly at far point) A( at age 10) = 14D
Similarly A(at age 40) = 100/25 – 1/ infinite= 4D.
Since, we usually keep the book at about 25cm so we can read comfortably up to the age of 40 years. After the age of 40 years near point of accommodation recedes beyond the normal reading or working range. This condition of failing near vision due to age related decrease in the amplitude of accommodation or increase in punctum proximum is called presbyopia.
Cause:- decrease in the accommodation power of crystalline lens with increasing age leading to presbyopia occurs due to
- Age related changes in the lens which include:
• decrease in the elasticity of lens capsule and
• progressive increase in size and hardness of lens substance which is less easily moulded. - Age related decline in ciliary muscle power may also contribute in causation of presbyopia.
Causes of premature presbyopia are:
• premature sclerosis of the crystalline lens
• uncorrected hypermetropia.
• chronic simple glaucoma
• general debility causing presenile weakness of ciliary muscle.
Symptoms:- 1. Difficulty in near vision:
Patients usually complaint of difficulty in reading small prints. Another important complaint of the patients is difficulty in threading a needle, etc.
- Asthenopic symptoms: due to fatigue of the ciliary muscle are also complained after reading or doing any near work.
- Intermittent diplopia: occurring due to disturbed relationship between accommodation and convergence may be experienced by few patients.
Treatment:- 1. Optical treatment: the treatment of presbyopia is prescription of appropriate convex glasses for near work.
Rough guide for providing presbyopia glasses in an emmetrope can be made from the age of the patient.
• 45 years: +1 to +1.25D
• 50 years : 1.5 to 1.75D
• 55 years : +2 to +2.25D
• 60 years : +2.5 to +3D
Exact presbyopia addition required should however be estimate individually in each eye in order to determine how much is necessary to provide a comfortable range.
Basic principles for presbyopia correction are:
• always find out refractive error for distance and first correct it.
• find out the presbyopia correction needed in each eye separately and add it to the distant correction.
• near point should be fixed by taking due consideration for professional of the patient.
• the weakest convex lens with which an individual can see clearly at the near point should be prescribed since overcorrection will also result in asthenopic symptoms.
Presbyopia spectacles may be unifocal, bifocal or varifocal, i.e progressive.
- Surgical treatment: various surgical methods have been proposed to treat presbyopia. The include monovision LASIK, conductive keratoplasty(CK) presbyopia LASIK, and more recently the corneal inlay. Beside these presbyopia clear lens extraction with multifocal Or accommodative intraocular lens (IOL) implantation. Anterior ciliary sclerotomy is another procedure proposed earlier.
Insufficiency of accommodation:
The term insufficiency of accommodation is used when the accommodative power is significantly less than the normal physiological limits for the patients age. Therefore it should not be confused with presbyopia in which the physiological insufficiency of accommodation is normal for the patients age.
Cause:- • early presbyopia
• weakness of the ciliary muscle due to general debility, anemia or toxemia.
• open angle glaucoma due to impairment of effectivity of the ciliary muscle by the increased intraocular pressure.
Symptoms:-
• eye strain
• difficulty with near work.
Treatment:-
• treatment of the cause
• reading spectacles (near addition)
• accommodation exercises.
Paralysis of accommodation:
Paralysis of accommodation also known as cycloplegia refers to complete absence of accommodation.
Causes:-
• unilateral
Cycloplegics( atropine)
Contusion of the eye
Paralysis of the third cranial nerve.
• bilateral
Diphtheria
Syphilis
Diabetes
Alcoholism.
Mydriasis usually accompanies the paralysis of accommodation. The prognosis is good in cases due to drugs or dipththeria. In trauma the condition may be permanent.
Treatment:-
• treatment of the cause
• if the paralysis is permanent suitable convex glasses may be prescribed
• miotics are seldom useful.
Spasm of accommodation:
Spasm of accommodation refers to exertion of abnormally excessive accommodation.
Causes:-
• found mainly in children, who attempt to compensate his refractive error.
• myopes are more affected than hypermetropes.
• may occur artificially by instillation of miotics.
• neurotic individuals who converge excessively.
Symptoms:-
• asthenopia
• blurring for distant vision.
Treatment:-
• atropinization for a few days Or weeks.
• assurance if necessary psychotherapy.







{kind=link}