
A sensory motor examination consists of multiple measurements of the ocular alignment positions and may include tests of fusion and binocular (3D) vision. A sensory evaluation detects, assesses, monitors, & manage strabismic conditions including esotropia, exotropia & hypertropia.
Normal Binocular Development :
- Binocular sensitivity and binocular fusion are absent at birth.
- Afferent from each eye segregate in LGN and 4c layer of ocular dominance columns (ODC) of striate cortex.
- Horizontal binocular connections develop between ODC’s of each side are weak at birthand become sharply defined at 3-6 months of age.
- Stereopsis emerge in humans during the first 3-5 months of post natal age.
Binocular single vision :
- Binocular single vision (BSV) is the ability to use both eyes together to achieve a single fused percept, even in the presence of disparity of the image seen by each eye.
- This represents the highest form of binocular cooperation.
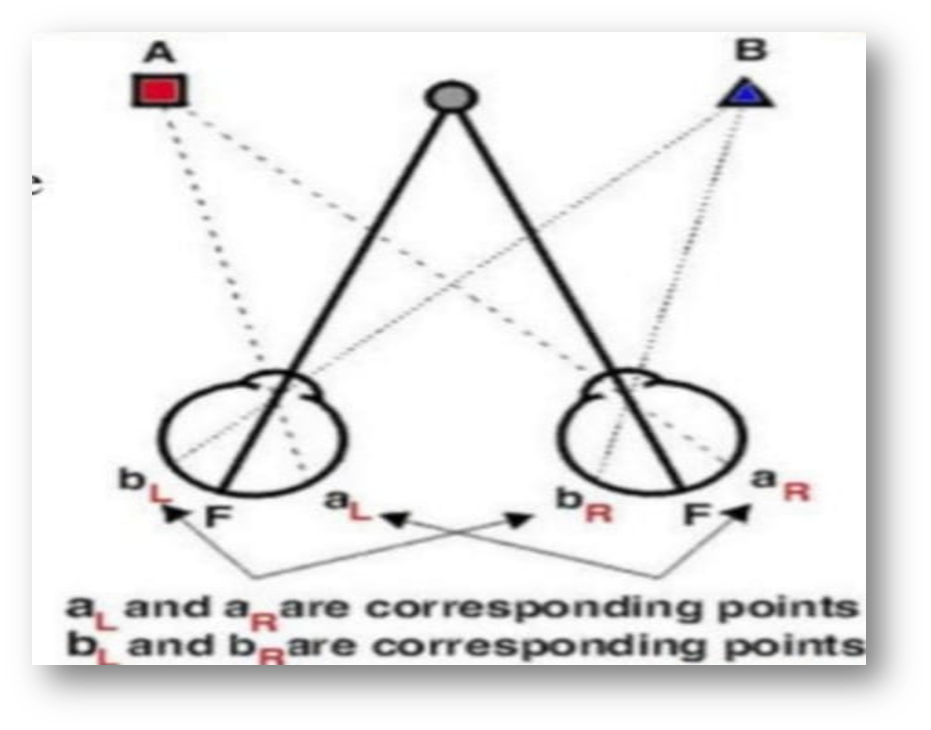
CORESPONDING RETINAL POINTS :
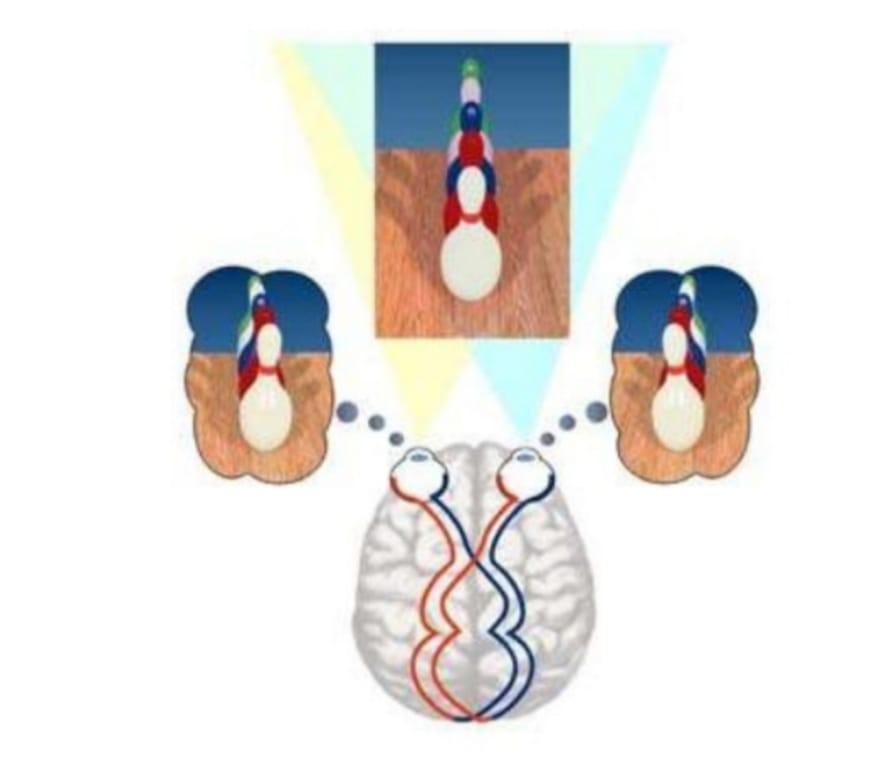
- Corresponding retinal points are points stimulated on the retina that give rise to the same visual direction. When objects stimulate non-corresponding points, this gives rise to different visual directions. These retinal points are called disparate points.
- Image from each eye is superimposed on each other in occipital cortex to obtain binocular single vision.
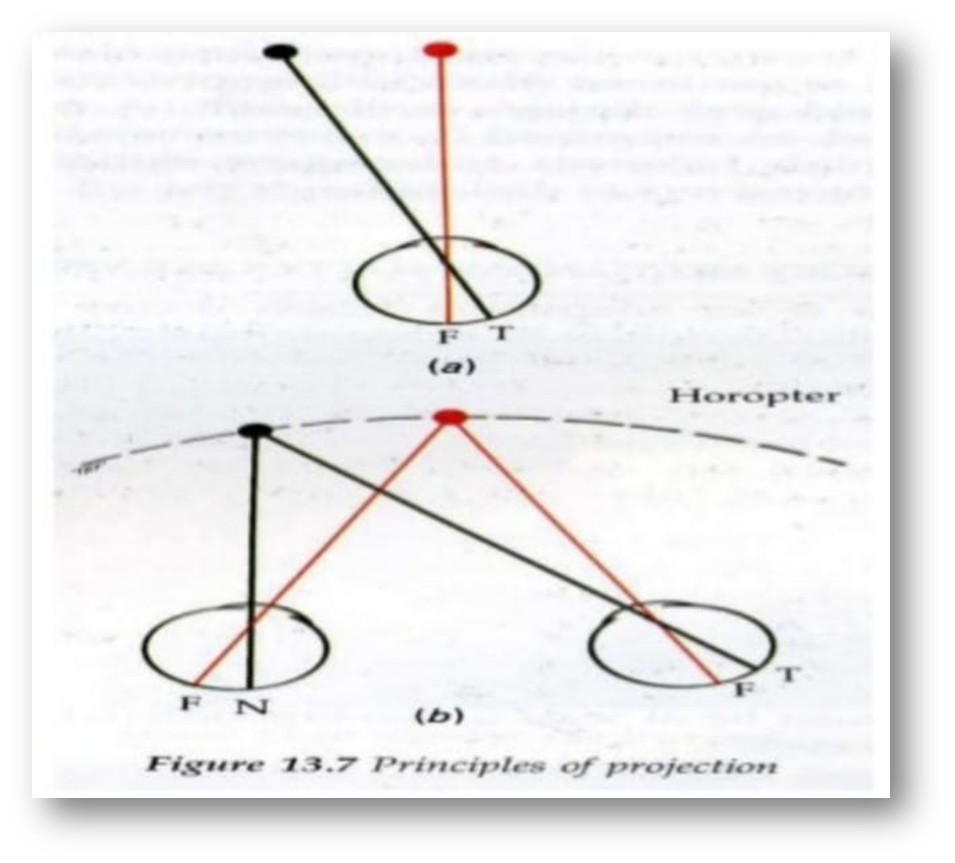
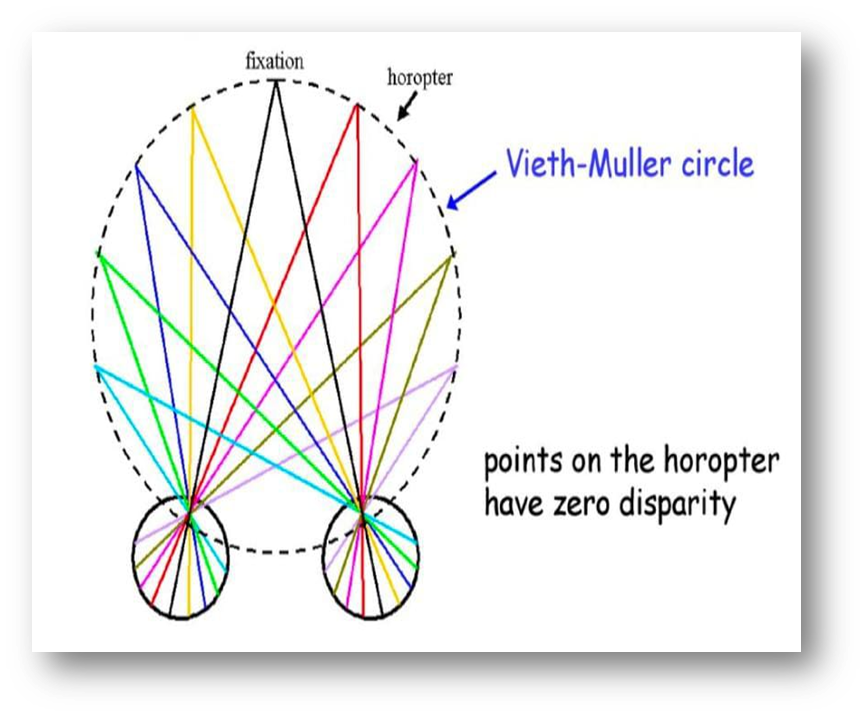
HOROPTER :
The locus of object points in space that stimulate corresponding retinal points of the two eyes when the eyes are fixating binocularly one of these object points. The horopter is a curve that passes through the fixation point and changes shape with fixation distance. Objects closer to the eyes than the horopter are seen double (crossed disparity) and objects further than the horopter are seen double (uncrossed disparity).
PANUMS’ FUSIONAL AREA :
- The region around the horopter that’s allows single vision.
- Objects stimulates slightly non-corresponding points.
- Objects are not only seen single, but are seen stereoscopically.
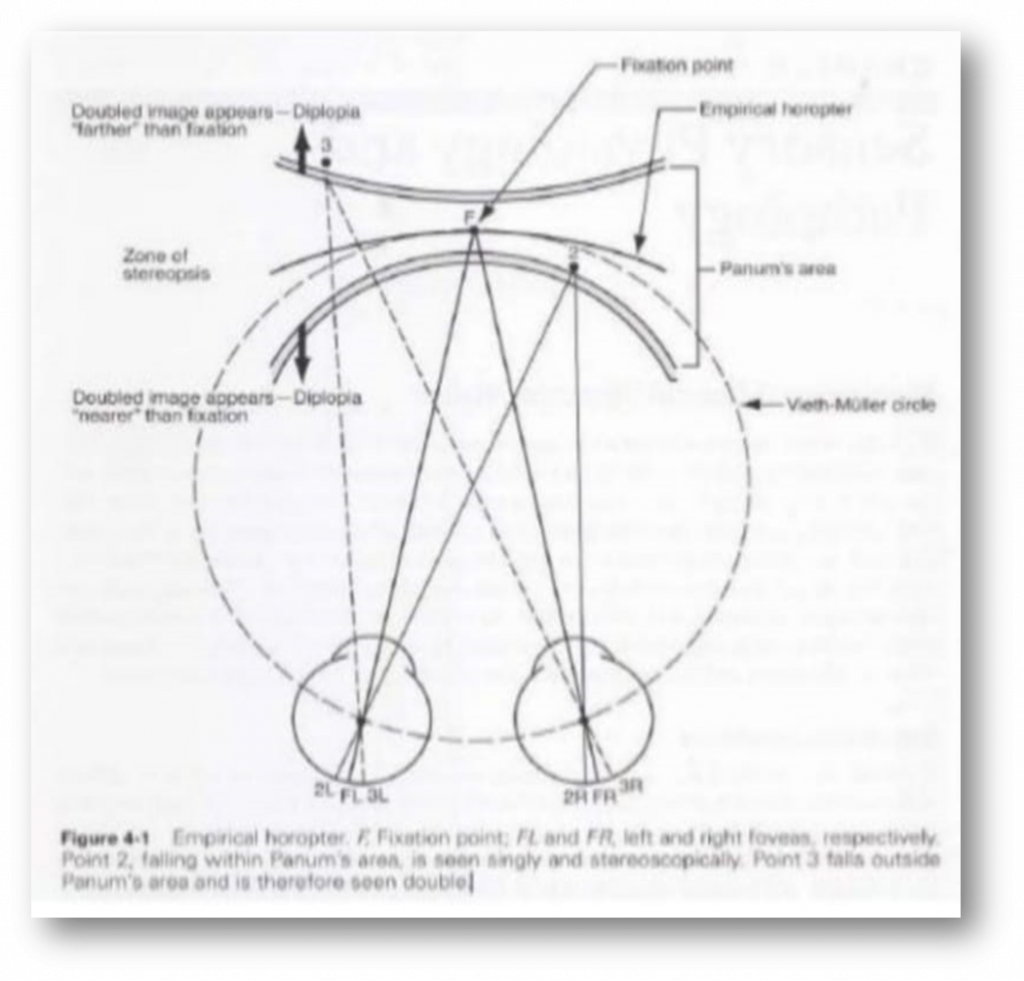
Physiological diplopia :
The diplopia elicited by an object off the Panum’s fusional area.
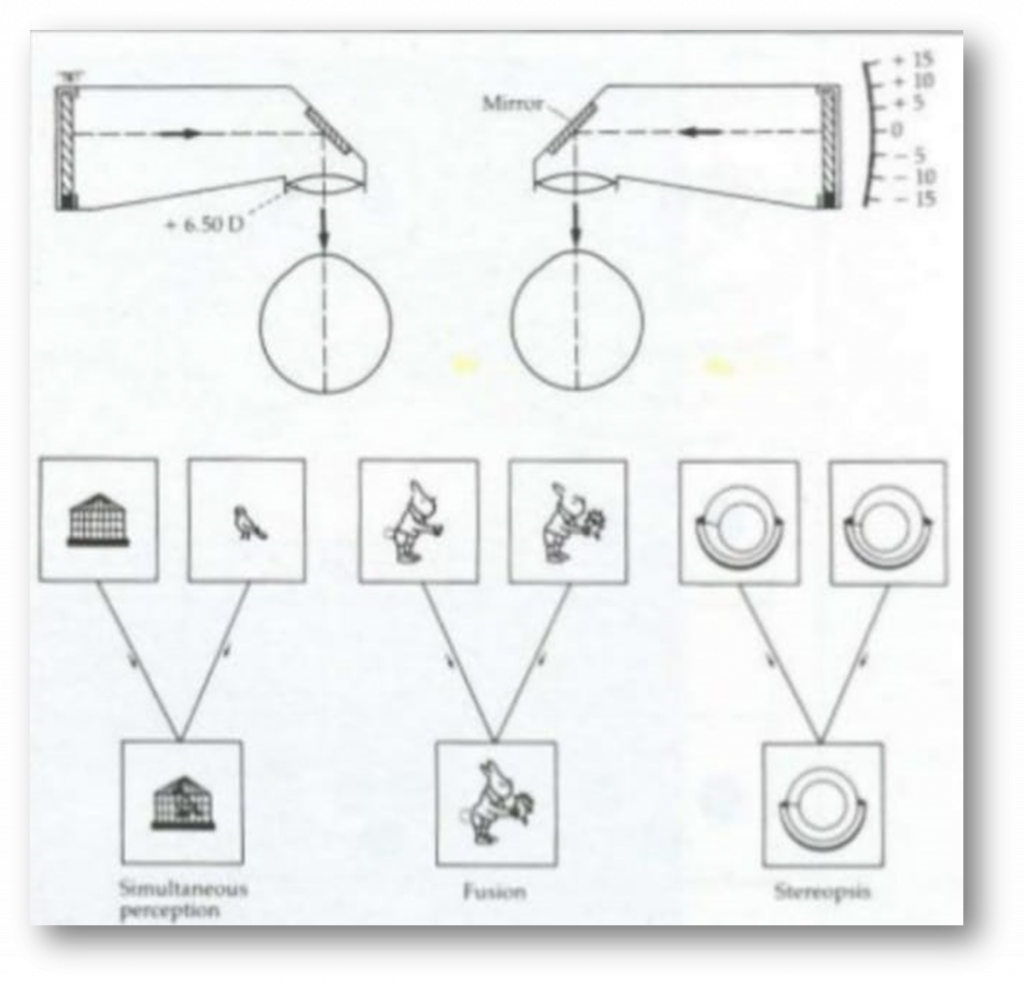
Grades of binocular vision :
- Simultaneous perception :
- It is the most elementary type of binocularity.
- Occurs when visual cortex perceives separate stimuli from the two eyes at the same time and concerns itself essentially with the absence of suppression.
- Superimposition :
- The two different pictures are seen simultaneously in the same direction
- Differing targets are the superimposed into one.
- SENSORY fusion :
- The neural process by which images in each retina are synthesized or integrated into a single percept. In normal BV, this process occurs when corresponding regions of the retina are stimulated.
- This is a cortical action.
- Stereopsis :
- It is the ability to fuse images that stimulate horizontally disparate elements within Panum’s fusional area resulting in binocular appreciation of visual object in depth i.e. in the third dimension.
- Stereopsis occurs when retinal disparity is large enough for simple1 fusion but small enough not to cause diplopia.
Abnormal Binocular vision :
- Sensory adaptation :
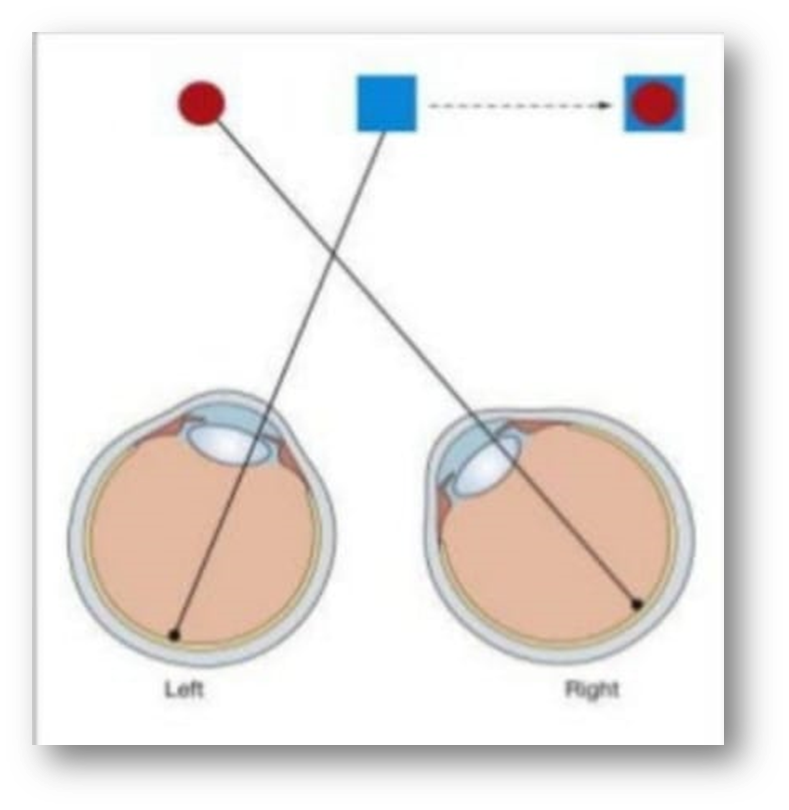
Confusion :
Simultaneous appreciation of two superimposed but dissimilar images caused by simulation of corresponding retinal points by images of different objects.
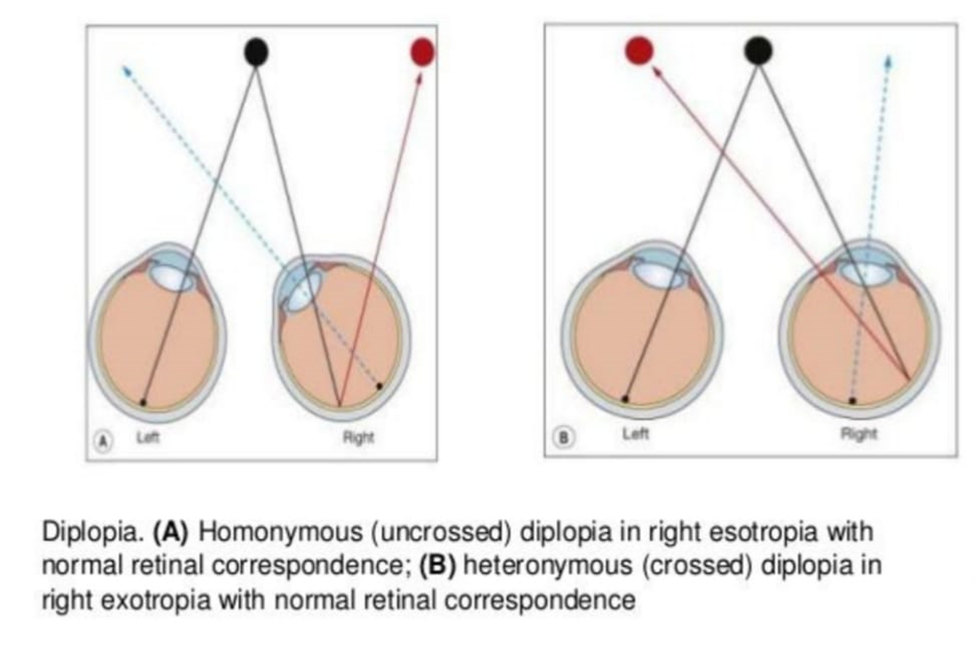
Diplopia :
Diplopia is the simultaneous perception of two images of a single object that may be displaced horizontally or vertically in relation to each other. Also called double vision, it is a loss of visual focus under regular conditions, and is often voluntary. However, when occurring involuntarily, it results in impaired function of the extraocular muscles, where both eyes are still functional, but they cannot turn to target the desired object. Problems with these muscles may be due to mechanical problems, disorders of the neuromuscular junction, disorders of the cranial nerves (III, IV, and VI) that innervate the muscles, and occasionally disorders involving the supranuclear oculomotor pathways or ingestion of toxins.
Suppression :
- Cortical inhibition of visual sensation that originates from spatially abnormally eye to eliminate the problem of visual confusin and diplopia.
- Pathplogic suppression results from strabismic misalignment of the visual axis.
- Physiologic suppression occur in eyes with BSV.
PATIENT WITHOUT SUPPRESSION :
TYPES OF SUPPRESSION :
- Central/Peripheral :
- In central suppression the image from the fovea of the deviating eye is inhibited to avoid confusion.
- Diplopia is eradicated by the process of peripheral suppression, in which the image from the peripheral retina of the deviating eye is inhibited.
- Monocular/alternating :
- Suppression is monocular when the image from the dominant eye always predominates over the image from the deviating eye, so that the image from the latter is constantly suppressed. This type of suppression leads to amblyopia.
- When suppression alternates amblyopia is less likely to develop.
- Facultative/obligatory :
- Facultative suppression occurs only when the eyes are misaligned eg. Intermittent exotropia.
- Obligatory suppression is present at all times, irrespective of whether the eyes are deviated or straight.
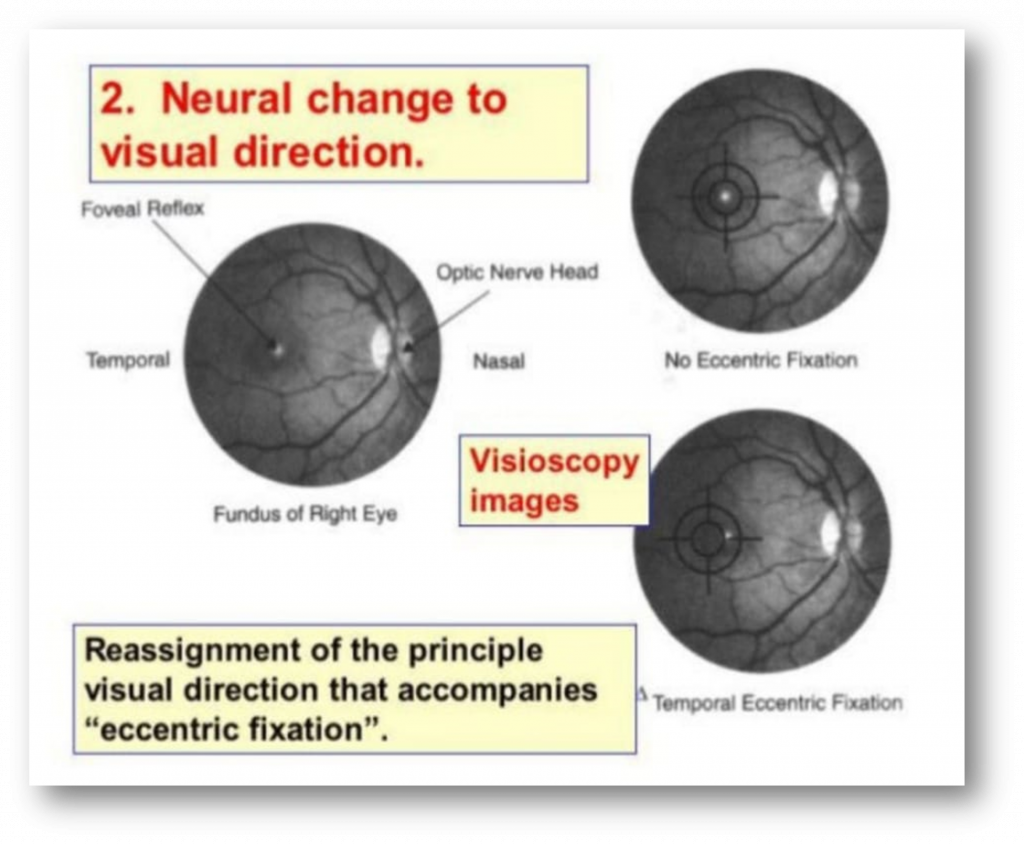
Ecentric Fixation :
- The fovea has lost its principal visuall direction
- Looking straight at an abject stimulates non foveolar retinal area.
Types :
Foveal off center :- 1 degree or less
Parafoveal :- 3 deggres or less
Paramacular :- 5 degree or less
Peripheral :- Greater than 5 degrees
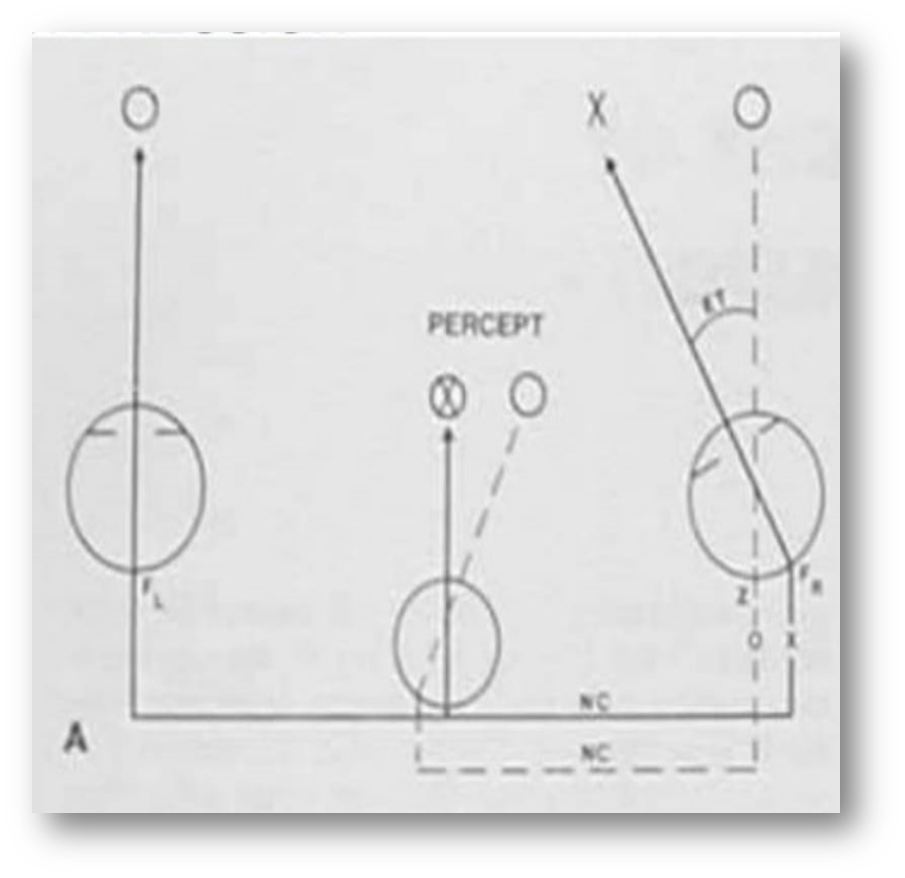
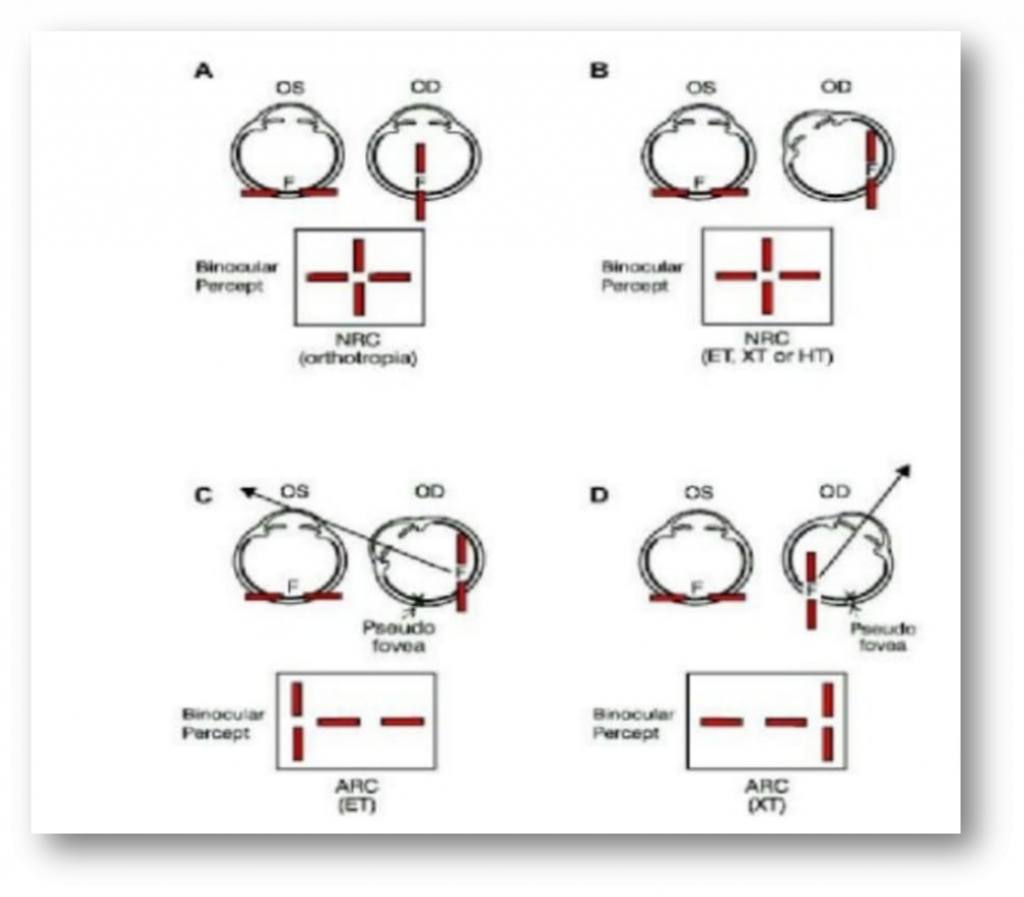
Abnormal retinal correspondence (ARC) :
In abnormal retinal correspondence (ARC) — also known as anomalous retinal correspondence , there is an eye turn, known as strabismus. In this situation, the fovea of the turned eye is not looking at the object. This would usually cause double vision, which is very disabling. To stop the double vision (diplopia), the brain ‘turns off the original fovea’ and creates a new point in your retina, called an extra-fovea or a faux-fovea, to compensate for the misalignment.
TESTS FOR SENSORY ANOMALIES :
- Visual acuity
- Worth four dot test
- Bagolini’s test
- 4 prism base out test
- Synaptophore
- After image test
- Visuoscopy
- Test for stereopsis
VISUAL ACUITY :
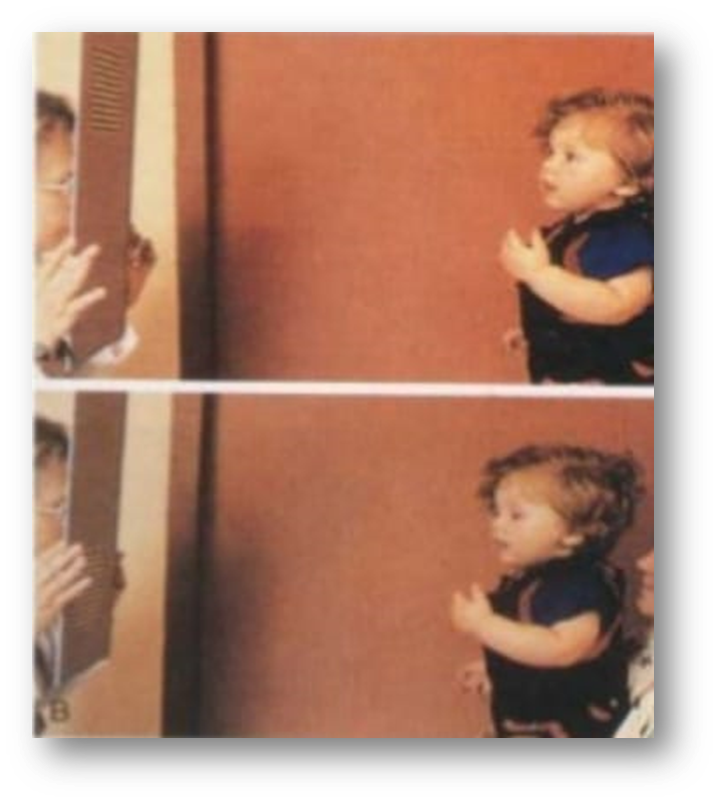
Fixation behavior test :
- Test is performed by seating the child comfortably in mothers lap.
- Object, usually a bright colored toy is slowly moved to the right and to the left.
- If the baby can hold fixation on the target and follow it when the target moves, the visual acuity noted as fix and follow behavior.
- Each eye is tested separately.
CSM method rating monocular fixation :
Done with one eye fixation on a target held at 40 cm.
Vision is noted as noted as CSM if –
C (central) – If each eye fixates centrally, the light reflex is seen in the center of the pupil.
S (steady) – Holds steady fixation on the target when it is moved.
M (maintained) – Continues to stay fixated on the target even if occlusion is removed from the follow eye.
2. Preferetinal looking test :
- Two fields are shown to infant one has a striped pattern and the other one is homogenous.
- Examiner is hidden behind the screen and is able to look through a hole in the screen at the infants eye.
- Infants tends to look more at the striped pattern.
- It is 6/240 in newborm
6/60 at 3 months
6/6 at 36 months
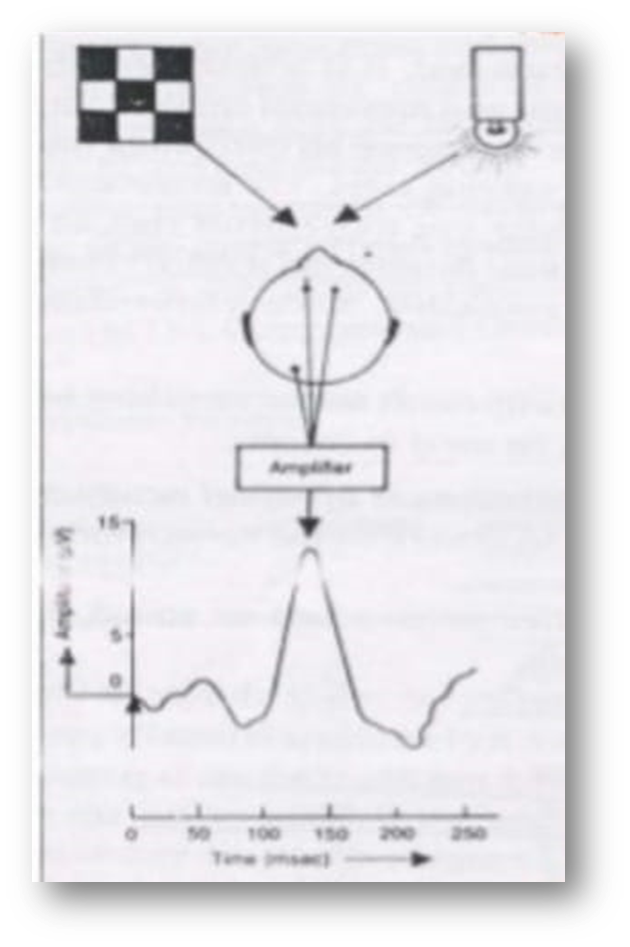
Visually evoked response (VER) :
- VER refers to electro-encephalographic recordings made from the occipital lobe in response to visual stimuli.
- It tells about the integrity of macular & visual pathway
- Pattern reversal VER is recorded using patterned stimulus as in checkerboard.
- Flash VER is recorded using flash light as stimulus.
- It is 6/120 at 1 month
6/60 at 2 months
6/6 – 6/12 at 1 year
VISUAL ACUITY :
- At age 2 years, picture naming test such as the crowded kay pictures.
- At age 3 years, most children will be able to undertake the matching of letter optotypes as in the keeler logMAR.
- Older children – Snellen’s , LogMAR chart.
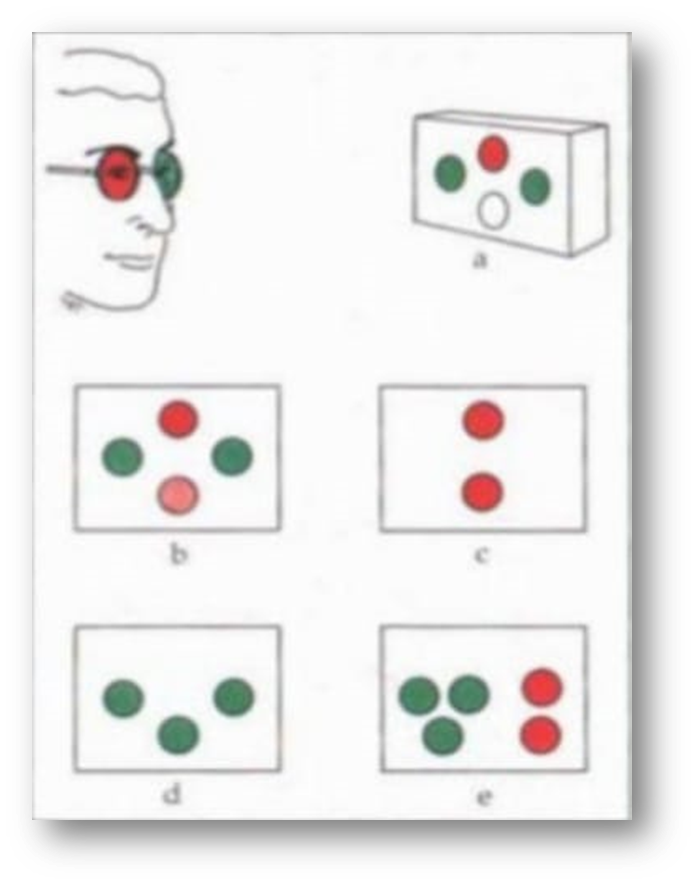
WORTH FOUR DOT TEST :
- A gross test which provides information only about the status cooperation.
- Can be used for distant and near fixation.
- Homononious ARC = 4 lights (deviation)
- 2 lights (Left suppression)
- 3 lights (Right suppression)
- 5 lights (Diplopia)
Bagolini striated glasses :
Bagolini striated glasses are glasses of no dioptric power that have many narrow striations running parallel in one meridian. These glasses cause the fixation light to appear as an elongated streak perpendicular to the striations. The lenses are usually placed at 135 degrees in front of the one eye and at 45 degrees in front of the other. Each eye receives a similar, fusible image, with the exception of the line, allowing simultaneous perception to be observed. With both eyes, the patient should see a cross. This test is minimally dissociative for the assessment of retinal correspondence.Apart from testing binocular functions, Bagolini striated glasses can measure cyclotropia . The principle of the test is similar to that of double Maddox rod test. The glasses are placed in the trial frames with the striations vertical, giving rise to two horizontal line images when viewing a spotlight. If the patient has a vertical deviation, the lines will be seen one above the other. If there is little or no vertical separation, vertical prism can be used to separate the lines. The patient is asked if one or both lines are tilted. The lines can be straightened subjectively by rotating the glasses in the trial frame and the degree of cyclotropia recorded.


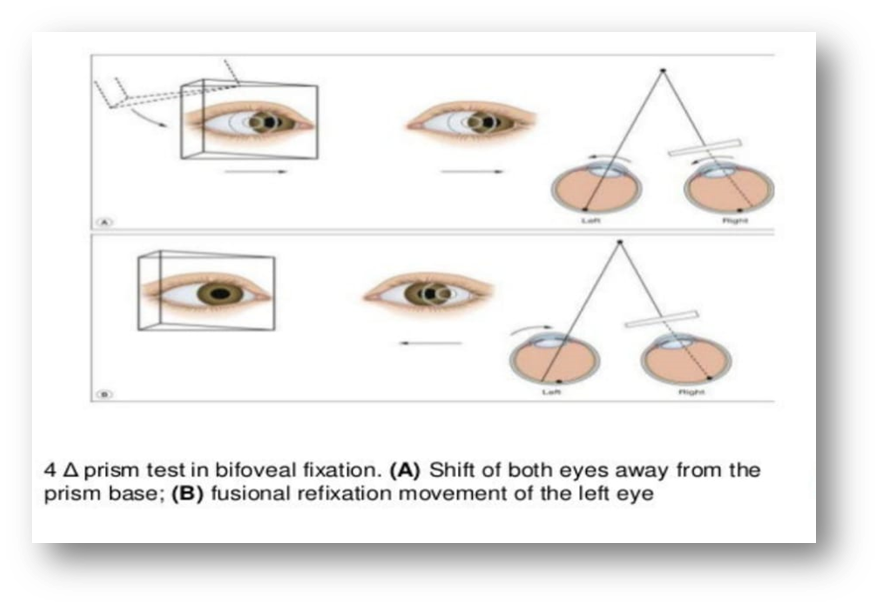
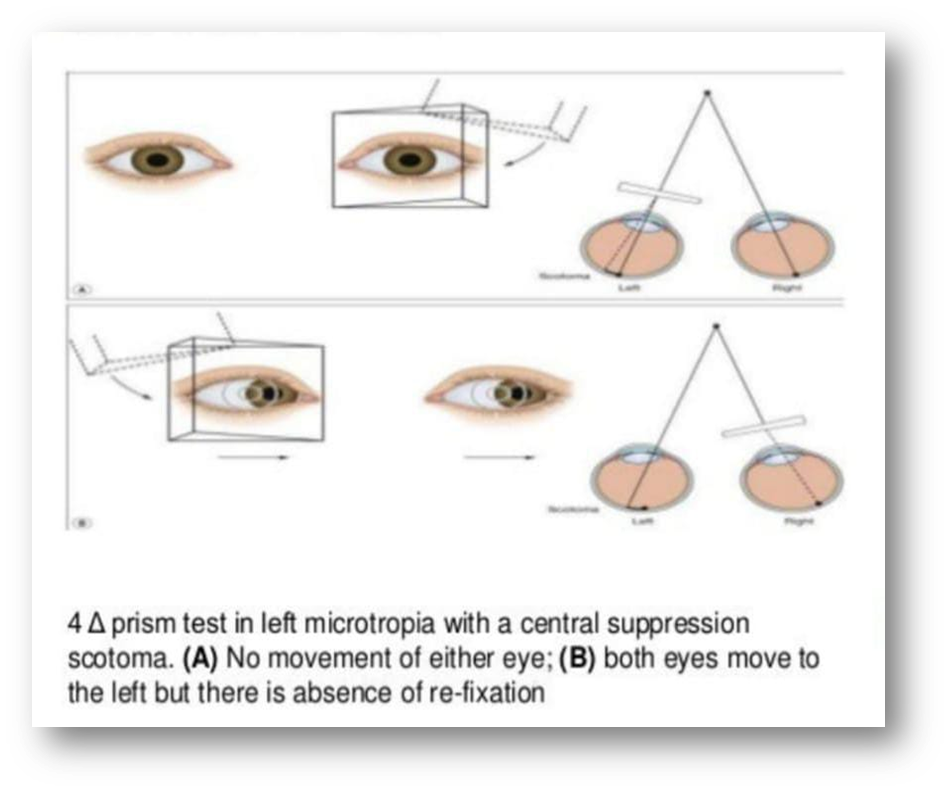
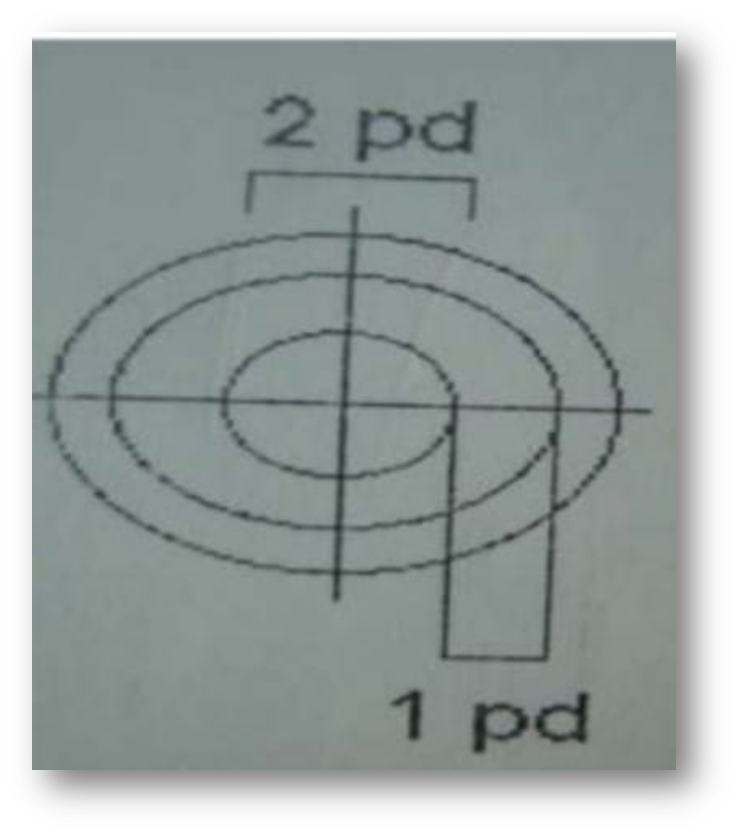
4 prism base out test :
- Usually determines whether a patient has bifocal fixation or a small suppression scotoma.
- A 4 prism dioptre base out prism is placed infront of one eye & a biphasic movement of the fellow eye is noted.

4 PRISM BASE OUT TEST FIG :
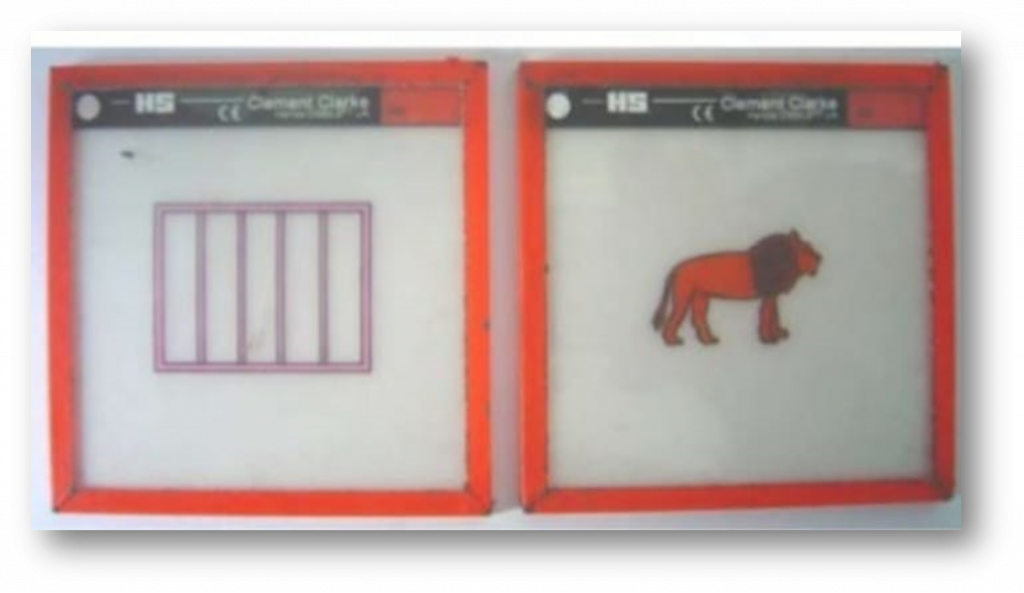
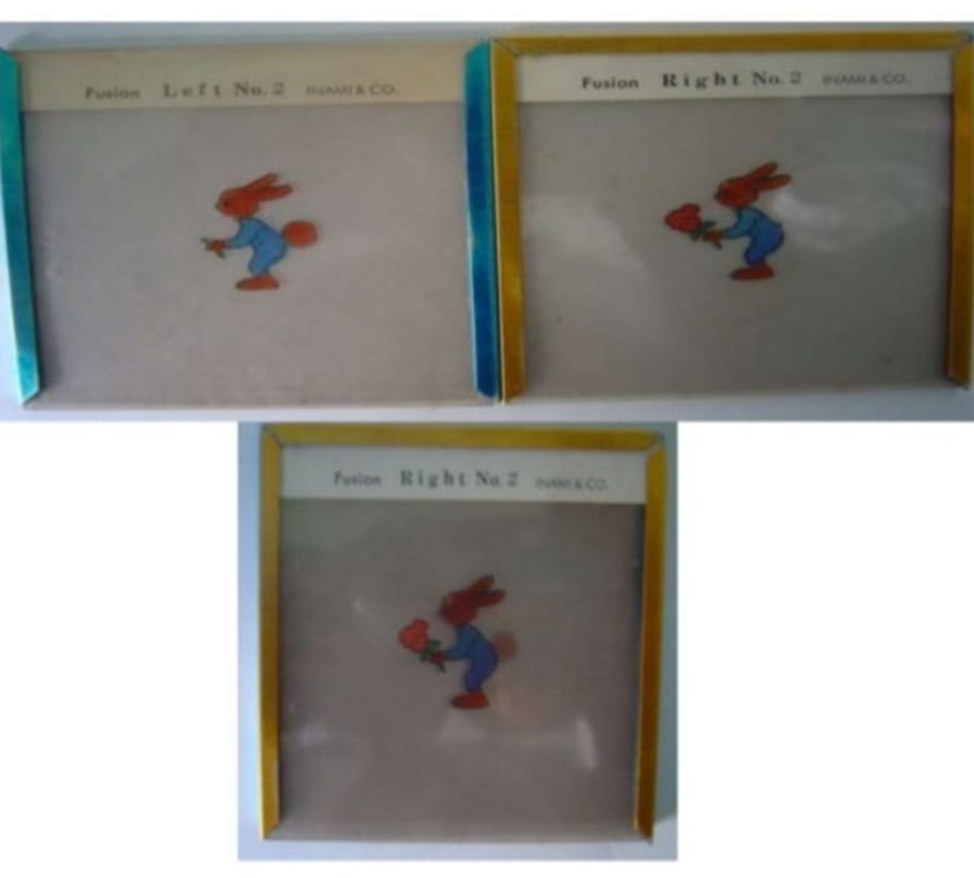
SYNOPTOPHORE :
An instrument for the assessment of strabismus and the grade of binocular vision.
AFTER-IMAGE METHOD (HERING -BEILSCHOWSKY TEST)
- In clinical practice the test is performed by using a battery-powered camera flash to produce a vertical afterimage in one eye and a horizontal afterimage in the other eye.
- Resulting after-image is that of a line with a break in its middle, which represents the fovea.
- The patient fixates steadily the central mark, first with one eye while the slit is horizontal and then with the other eye while the slit is vertical.
- In a darkened room or with the eyes closed, the patient sees the two successively imprinted as positive afterimages (bright lines)
- In a lighted room or with the eyes open, negative afterimages (dark lines) will be seen.
- Then open eyes and look at a plain surface and see if lines cross.
- In NRC the after images will coincide.
- In ARC the after images will be separated.
VISUOSCOPY :
Test of eccentric fixation available in opthalmoscope.
TESTS FOR STREREOPSIS :
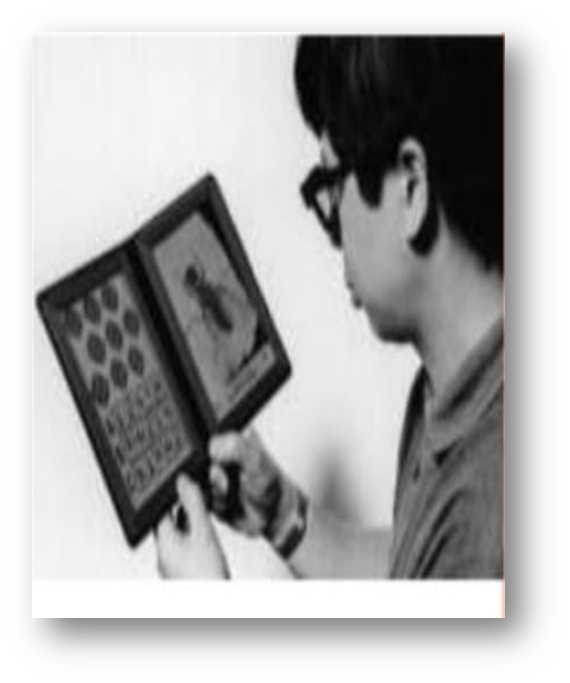
TITMUS STREREO TEST :
- The titmus test consists of a three dimensional Polaroid vectograph consisting of two plates in the form of a booklet viewed through Polaroid spectacles.
- The test is performed at a distance of 40 cm.
- Fly is a test of gross stereopsis (3000 seconds of arc), and is specially useful for young children.
- The fly should appear to stand out from the page and the child is encouraged to pick up the tip of one of its wings between finger and thumb.
- In the absence of gross stereopsis the fly will appear as an ordinary flat photograph.
- Circles comprise a graded series which tests fine depth perception.Each of the nine squares contains four circle.
- One of the circles in each square has a degree off disparity and will appear forward of the plane of reference of the presence of normal stereopsis. The disparities measured range from 800 to 40 sec of arc.

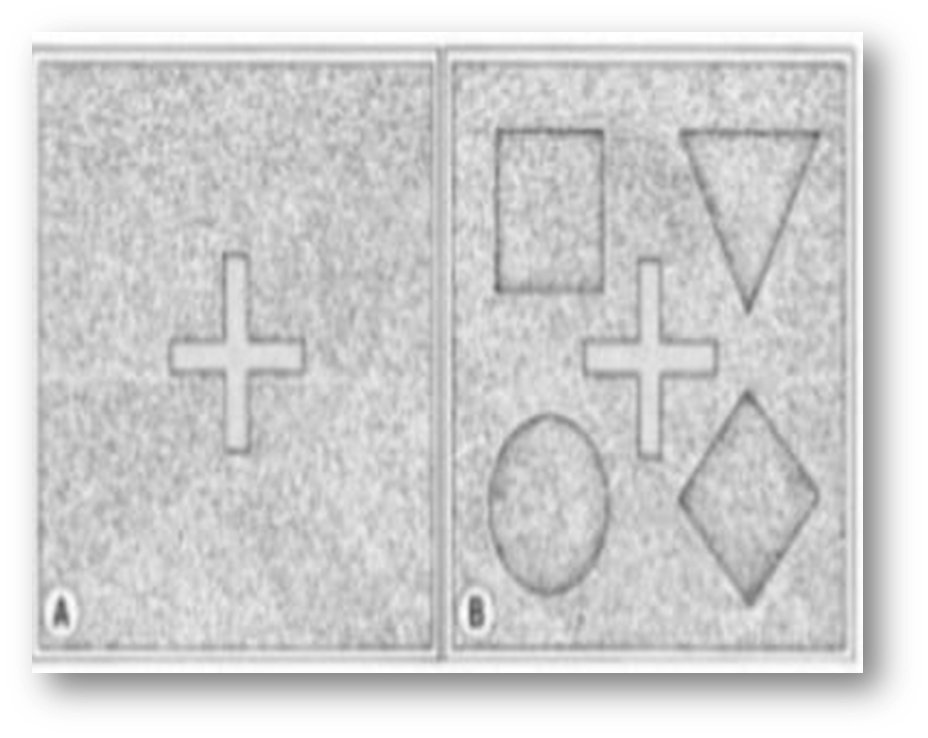
TNO RANDOM DOT STEREOTEST :
- The TNO random dot test consists of seven plates of randomly distributed paired red and green dots which are viewed with complementary red-green spectacles.
- Within each plate the dots of one colour forming the target shape (squares, crosses etc.) are displaced horizontally in relation to their paired dots of the other colour so that they have a different retinal disparity from those outside the target.
- Some control shapes are visible even without red-green spectacles while the test targets are only visible to an individual with stereopsis, while wearing red-green spectacles.
- The first plates are used to establish the presence of stereoscopic vision and subsequent plates to quantify it.
- Because there are no ore monocular clues, the TNO test provides a truer positive measurement of stereopsis than the titmus test, but can give false negative errors when fusion is poor.
- The disparities measured range from 480 to 15 sec of arc tested at 40 cm.
Most children are able to do this (and the Frisby test) from about 4 years of age.
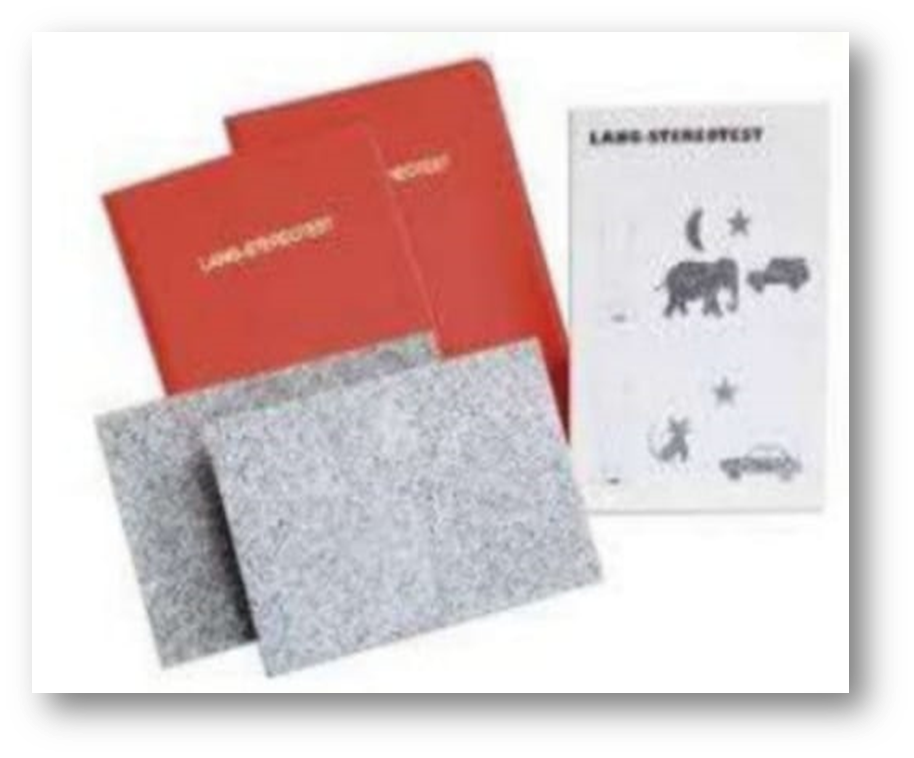
LANG STEREO TEST :
Lang I is a stereo test based on a combination of the random-dot technique and cylindrical gratings, consisting of a card measuring 9.5 cm ×14.5 cm that contains pictures of a cat, a star, and a car, which represent disparities of 1200, 600, and 550 seconds of arc, respectively. The test is administrated at 40 cm of distance; it does not require red/green or cross-polarized filters. Incorrect naming or no identification of one or more stereoscopic figures was considered a fail (Lang I cut-off). We consider the test negative when patients named “dog” pointing to the image of the cat. Lang II stereo test is based, as well, on the random-dot technique. It consists of a card measuring 9.5 cm ×14.5 cm that contains pictures of an elephant, a car, and the moon, which represent disparities of 600, 400, and 200 seconds of arc, respectively. Similar to Lang I, the test is performed at 40 cm distance. This stereo test contains a control figure (a star), which is visible monocularly. The test does not require red/green or cross-polarized filters. Patients who usually wear prescription glasses have to use them during the test. Incorrect naming or no identification of one or more stereoscopic figures was considered a fail (Lang II cut-off). We considered the test negative when patients responded “turtle” pointing to the car or when the elephant was named as a “bear” or “cow”.







{kind=link}