

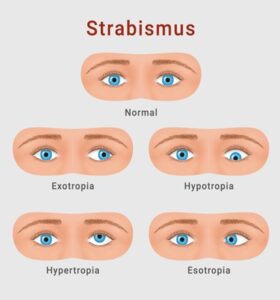
When a normal eye loses its alignment of parallelism and fixation of vision ,then it is called squint or strabismus.
This type of abnormalism can be described and evaluated by 2 components , and these are
1. Sensory component
2. Motor component
Motor connection of eye muscles can be remembered by a formula –
All 3 LR 6 SO 4
That means out of 6 extra ocular muscles , superior oblique is supplied by Trochlear nerve , Lateral rectus is supplied by Abducent nerve , and rest of the muscles are supplied by oculomotor nerve .
1.Oculomotor connection –

From the above diagram we come to know that , if oculomotor nerve is depressed then there can be ptosis, and ipsilateral (Weber syndrome ) or contralateral (Benedict syndrome) nerve palsy , or in other word down and out movement of eyeball .
2.Trochlear connection –

Above diagram depicts that if any depression affect the trochlea nerve ,that will cause intorsion , depression of eye ball and lateral rotation of it .

So to bring their visual axis in same line ,and to avoid diplopia , the patient have to bend his / her neck in one side with chin attached to collar bone .
Abducent nerve connection –

QAnd palsy of this nerve causes lateral rectus damage and that will cause uni or bilateral internal strabismus and furtherly that will cause diplopia. To evaluate the motor component palsy clinically we have to do some routinely tests , these are
1.Corneal reflex test ( Hirschberg) – In this test a flash of light is shone on the pupils to detect the gross position of the eyes. If the light reflex is towards the nasal side it is suggestive of divergent squint (eye is deviated outwards), if it is towards the lateral side it is suggestive of convergent squint (eye is deviated inwards).

2.Cover test – This test is done to confirm the direction of manifest squint. The apparently normal eye is covered to see the movement of the squinting eye. If the eye moves inwards towards the nose it suggests a divergent squint, if it moves away from the nose it suggests a convergent squint, if the eye moves downward it indicates an upward deviation of the eye, if the eye moves upward it suggests a downward deviation of the eye.
3.Uncover test – In this test the movement of the eye that is covered is studied too see any hidden latent squint.

4. Alternate cover test – Either eye is occluded to see the visual fixation in each eye as well to detect any presence of lazy eye depending on the preference of fixation.
5.Motor function test – The patient is asked to follow a target in nine different directions of gaze to assess the action of the extraocular muscles. This enables the ophthalmologist to decide which muscle is overacting or underacting.

6.prism cover test – This test is done to quantify the amount of squint. A special prism glass is placed on the eye in increasing amounts to neutralize the deviation which gives the ophthalmologist a measure of the squint. This may be done in various gazes to measure the squint in different directions.

These tests are always accompanied by other routine eye checking tests like checking vision, glass powers and a detailed evaluation of the front as well as the back part of the eye. The advice about the squint is based on this comprehensive examination.
Based on this evaluation, squint specialist determines the next steps in managing the squint which may vary from glass prescription to eye patching to an actual eye surgery for squint correction.
Two red notices –
As motor function , any depression in facial nerve can cause abnormal face expression and non-closure of eye lids .
As motor function , any depression in Trigeminal nerve can cause sudden sporadic ,shock like appearance around the eye .







{kind=link}