
Esophoria is the tendency to converge or deviate inward. the smaller degrees of esophoria is extremely common and as a rule, they do not give rise to any symptoms. But when the deviation is more than 5 degrees, there is usually some amount of distress.
Phorias are misalignment that only occurs some of the time, such as when the synchronization between the eyes is broken by covering one eye. Basically, phoria is a tendency to deviate but that is prevented by the fusion mechanism for the interest of BSV. But under the condition of stress, or when the fusion is interrupted the deviation readily becomes manifest.
A large proportion of esophoric conditions have problems with accommodation as their root cause. Due to the synergistic link between accommodation and convergence, excessive accommodation produces excessive convergence and thus esophoria. However, a small proportion of esophoric conditions may be classed as non-accommodative i.e, faulty accommodative – convergence plays no part in the condition.
Types of esophoria
- Convergence excess type- esophoria is greater for near distance.
- Divergence weakness type – esophoria is larger for distance than near.
- Nonsignificant type or Basic type – where esophoria is relatively equal for near and distance.
AETIOLOGY:
- Uncorrected hypermetropia is the most common cause of esophoria in distance vision and in this accommodative esophoria spectacle correction usually helps reduce the magnitude of the phobias.
- Muscle tonus in the adductors may be a factor in esophoria in young patients.
- High AC/A ratio
- Weak negative fusional reserves
- Anatomical factors such as enophthalmos, narrow IPD, EOM anomalies
General factors –
a) endocrine overactivity
b) diseases of the CNS
c) anoxemia- lack of oxygen
SYMPTOMS
- The blurring of vision, especially at times of fatigue. Initially, with an effort of fusion, this blurring may be overcome.
- Headache and eye ache (strains) are extremely common.
- Intermittent diplopia due to exhaustion of fusional reserve intermittently.
- Difficulty changing focus.
DIAGNOSIS
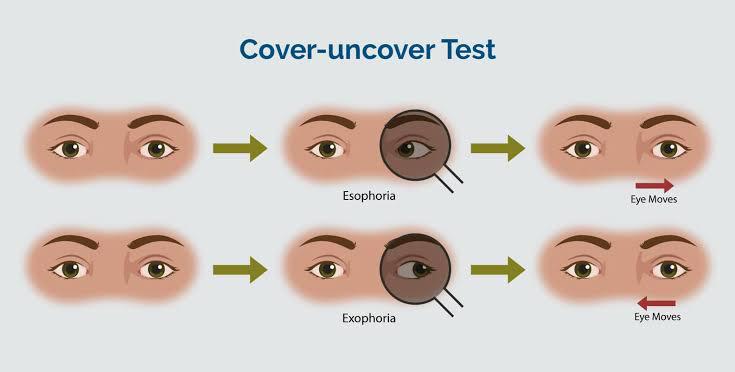
Cover test – one eye is covered and the other eye is made to fix on an object. In presence of esophoria, the eye under cover deviates temporally. When the cover is removed, the covered eye corrects the deviation, and regains its normal position quickly. cover test should be performed for both near and distance using accommodative targets.
Maddox rod test – it consists of a series of parallel high power, plus cylinders, that convert a point light into a red straight line, at the right angle to the axis of the rod. When the Maddox rod is held in front of one eye, the images of the point source of light in 2 eyes become dissimilar and fusion becomes dissociated. This test is performed at a distance of 6M and 33cm.
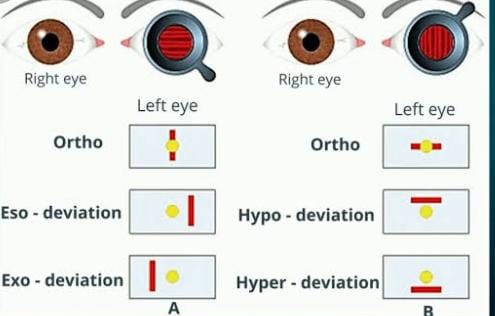
In heterophoria, the red line of light becomes separated from the point source of light.
Maddox wing test – dissociates the eyes for near fixation. Done at 33cms. The principle used here is the dissociation of fusion by dissimilar objects.
Prism vergence tests – the strength of the involved muscles is to be tested by forcing them to the maximum effort against the prism.
Synaptophore evaluation – to know the range of fusion.
MANAGEMENT OF ESOPHORIA
Smaller degrees of esophoria which give rise to no symptoms require no treatment. Indications for treatment include
- Symptoms producing deviation
- Children, where there is the possibility of decompensation in later life.
- Circumstances where it is necessary to achieve specific standards for certain careers.
AIMS of treatment include
- Reducing the deviation within the fusional amplitude.
- Improving fusional vergence.
- Improving fusional amplitude.
TREATMENT
- Refractive errors must be corrected fully by spectacles, which should be worn constantly. Cycloplegic refraction is required in case of convergence excess to explore the possibility of latent hypermetropia, spasm of accommodation, and pseudo myopia. Bifocals are prescribed for young patients with convergence excess. Bifocals are contraindicated in cases of low AC/A ratio.
- Orthoptic exercises – for esophoria, it is important to improve negative relative convergence with stereograms using distance fixation, bar reading, and exercises with base-in prisms and the divergent range on synaptophore.
- Prisms – may be used with moderate or large angle deviations. The deviation should be only partially corrected (often half the prism cover test measurement) so that fusional vergences continue to be exercised. the base of the prism is placed on the opposite side of the direction of deviation and the power is equally divided between the two eyes.
- Surgery – rarely indicated. With moderate or large angles it may be necessary to reduce the angle surgically as fusional vergences may not be sufficient to maintain comfortable control at all times.
- Botulinum toxin – can be used both diagnostically and therapeutically and a single administration may be sufficient to allow a return to asymptomatic BSV. Injection to MR is undertaken for esophoria.
Sources –
- Essentials of ophthalmology ( SK Basak)
- Clinical orthoptics(Fiona J Rowe)
- Binocular vision and orthoptics (AK Khurana)







{kind=link}