

Asthenopia is a term used to describe a sense of strain and weakness or ocular fatigue set up by the use of the eyes (a = not, sthenos = strengh, ops = vision) (Atencio 1996, Palmer 1993). Asthenopia is a common presenting complaint among patients with accommodative and convergence insufficiency, refractive errors and intermittent strabismus.

Asthenopic symptoms are less frequent at distance vision than at near vision, because there is less strain on the accommodation and vergence systems. Asthenopia symptoms are becoming more common in modern society where near work at computers require sustained fixation, often for hours, at the same visual distance, which puts a strain on the system for near vision However, also in schoolchildren asthenopia can occur, and recent studies report a prevalence of 15.2% in 6 years old children and 34.7% in schoolchildren 6-10 years old.
Asthenopia is also often caused by uncorrected refractive errors (hypermetropia, myopia, astigmatism and anisometropia), and the condition is then called refractive asthenopia . Asthenopic symptoms can be caused by neuromuscular anomalies and this form is termed muscular asthenopia(heterophoria, heterotropia and convergence insufficiency). Asthenopia due to disturbances of accommodation may be regarded as either refractive asthenopia or as muscular asthenopia.
- Refractive asthenopia B. Muscular asthenopia
- Muscular Asthenopia
Heterotropia
Heterophoria
Convergence Insufficiency
Accommodative Insufficiency
- Refractive Asthenopia
Hypermetropia
Myopia
Astigmatism
Anisometropia
Refractive Asthenopia
Hypermetropia:-
Hypermetropia is a condition in which distance objects are focused behind the retina when the accommodation is relaxed, i.e. the image is defocused unless the subject accommodates or wears convex lenses.
Hypermetropia can be categorized by the degree of the refractive error in low hypermetropia (≤ 2.00 D), moderate hypermetropia (2.25–5.00 D) and high hypermetropia (≥ 5.00 D) .
Hypermetropia does not always require correction because young patients can accommodate to overcome part or all of their refractive error, hence achieving good near and distance vision.
However, in most children with asthenopia due to hypermetropia the amplitude of accommodation is low in relation to their degree of hypermetropia, i.e. these children are not able to comfortably overcome their hypermetropia. In these children correction of hypermetropia will reduce the accommodative demand resulting in stable binocular vision, and a decreased level or elimination of the asthenopic symptoms.
Myopia :-
Myopia is a refractive condition of the eye in which the images of distant objects are focused in front of the retina when the accommodation is relaxed.
However, objects located at the dioptric distance equivalent to the degree of myopia will be focused on the retina. In order for myopic subjects to see objects in a distance clearly they need to wear a concave refractive correction.
Myopia of more than 1.00 D in preschool children should be corrected. In cases of high exophoria or intermittent exotropia, a prescription for fulltime wear of the full refractive error is recommended. In cases of esophoria at near or accommodative insufficiency, a plus lens addition for near can also be appropriate.
Astigmatism :-
Astigmatism is a condition of refraction in which the image of a point object is not projected as a single point but as two focal lines at different distances from the optical plane (the retina). Astigmatism can be present in combination with hypermetropia or myopia. The focal lines can be focused: 1) behind the retina (compound hypermetropic astigmatism); 2) in front of the retina (compound myopic astigmatism); 3) behind and in front of the retina (mixed astigmatism) 4) or one focal line on the retina while the other is either in front or behind (simple astigmatism). In the case of astigmatism the patient needs a cylindrical correction in order to obtain a point focused image. Generally, all astigmatic refractive errors larger than 0.25D should be corrected if asthenopic symptoms are present (Benjamin 1998). Correction of astigmatism in all patients including those with asthenopia improved the visual acuity and stabilised the input into the accommodative system, thereby eliminating or reducing the symptoms of asthenopia.
Muscular Asthenopia
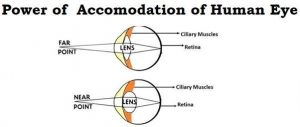
Accommodation :-
Accommodation is the ability of the ocular lens to change the refractive power in order to keep the image of the fixated object clear on the retina. Most visual problems associated with accommodation occur because accommodation is excessive, too low, or too slow.
The normal value of the near point of accommodation in relation to age is in cm (100/(18.5D – (0.3age).








{kind=link}