
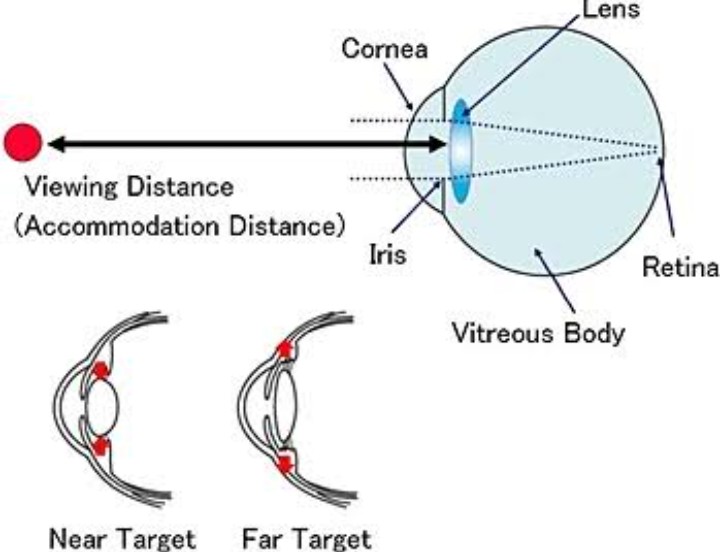
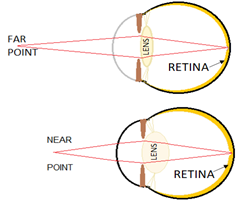
In ophthalmology, the term excessive accommodation is used to describe a situation in which an individual exerts more than the normal required accommodation (focusing on near object) for performing a certain near work. Accommodative excess has traditionally been defined as accommodation that is persistently higher than expected for the patient’s age. Using this definition, it is a rare condition to occur in isolation ( i.e., without being secondary to convergence insufficiency ). Modern definitions simply regard it as an inability to relax accommodation readily, one end of a continuum leading to frank spasm of accommodation. Using this newer definition, it is relatively common condition.
It is within the voluntary control of the individual and is an intermittent process, whereas the spasm of accommodation is continuous prolonged use of excessive accommodation.
Symptom and sign :
- Symptom:
- These symptoms are generally to the use of the eye for reding or other near tasks
- Long-Standing
- Blurred vision worse after reading or other close work
- Headache
- Eye strain
- Asthenopia
- Difficulty focusing from far to near
- Sensitivity to light
- Trouble concentrating when reading

- Signs:
- Direct measures of accommodative relaxation
- Difficulty clearing +2.00D with monocular accommodative facility
- Low monocular estimation method retinoscopy finding
- Indirect measures of accommodative relaxation
- Reduced negative relative accommodation
- Difficulty clearing +2.00D with binocular accommodative facility
- Low fused cross cylinder finding
- Low base-in to blur finding at near
Causes :
- Causes related to REFRACTIVE ERRORS :
- Young hypermetropes frequently use excessive accommodation as a physiological adaptation in the interests of clear vision.
- Young myopes performing excessive near work may also use excessive near work may also use excessive accommodation in association with excessive convergence.
- Astigmatic errors in young persons may also be occasionally associated with use of excessive accommodation.
- Presbyopes in the beginning use excessive accommodation to accomplish near work.
- Use of improper or ill-fitting spectacles may also cause use of excessive accommodation.
- Functional disorders to rule out
- Convergence excess
- Basic esophoria
- Accommodative insufficiency
- Accommodative infacility
- Nonfunctional causes of accommodative excess
- Causes related to systemic drug:
| Bilateral | Unilateral |
| DRUGS | LOCAL EYE DISEASE |
| Cholinergic drugs | None |
| Morphine | |
| Digitalis | |
| Sulfonamides and carbonic anhydrase inhibitors |
- Causes related to diseases :
| Bilateral | Unilateral |
| General disease | General diseases |
| ADULTS | Trigeminal neuralgia |
| Encephalitis | Head trauma |
| Syphilis | |
| Head trauma | |
| CHILDREN | |
| Influenza | |
| Encephalitis | |
| Meningitis | |
| Head trauma |
Risk factors: A large amount of near work is the main precipitating factor of accommodative excess.
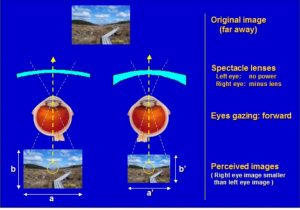
Pseudomyopia Pseudomyopia also known as artificial myopia refers to an intermittent and temporary shift in refractive error of the eye towards myopia. It may occur due to excessive accommodation or spasm of accommodation.
Diagnosis:
- Dynamic retinoscopy
- Cycloplegic refraction
- Parinaud’s syndrome
Treatment:
- Lenses Because uncorrected refractive error can be a cause of accommodative fatigue, we recommend that correction of significant ametropia be the first management consideration. When dealing with patients with accommodative excess even small degrees of refractive error may be significant. Prescribing for small degrees of hyperopia, astigmastism, and small differences in refractive error between the two eyes may provide some immediate relief of symptoms for the patient.
- Added Lenses Analysis of the near point findings in accommodative excess clearly shows that these patients Would not benefit from the use of added plus lenses. The low NRA , difficulty clearing plus during accommodative facility testing, the normal amplitude of accommodation, and low MEM retinoscopy are all examples of data suggesting that plus well not be helpful.
- Vision therapy A vision therapy program for accommodative excess generally requires 12 to 24 in-office visits, if vision therapy is office based. The total number of therapy sessions also depends on the age of the patient and his or her motivation and compliance.
- Objectives of Vision Therapy for Accommodative Excess
- Phase 1
- Develop a working relationship with the patient
- Develop an awareness of the various feedback mechanisms that will be used throughout therapy
- Develop feeling of diverging , looking away, relaxing accommodation
- Phase 2
- Normalize positive fusional vergence (PFV) amplitudes (smooth or tonic vergence demand)
- Normalize NFV facility at near (jump or phasic vergence demand)
- Normalize PFV facility (jump or phasic vergence demand)
- Phase 3
- Normalize NFV amplitudes at intermediate distances
- Normalize NFV facility at far
- Sample vision Therapy Program for Accommodative Excess
- Phase 1
- Sessions 1 and 2
- IN-OFFICE
- Discuss nature of vision problem, goals of vision therapy, various feedback cues, importance of practice
- Lens sorting
- Loose lens rock (begin with plus lenses)
- Brock string
- Tranaglyphs or vectograms: base-in
- Begin with a peripheral target such as tranaglyph 515 or the Quoit vectogram
- Computer Orthoptics Random Dot program: base-in

- Home Therapy
- HTS Accommodation program
- Loose lens rock
- Brock string
- Sessions 3 and 4
- IN-OFFICE
- Loose lens rock ;plus lenses
- Bug on string
- Tranaglyphs or vectograms: base- in
- Use targets with more central demand (clown, Bunny tranaglyphs; Clown, Topper vectograms )
- Computer Orthoptics Random Dot Program: base-in
- HOME THERAPY
- HTS Accommodation program
- Loose lens rock
- Bug on string
- Sessions 5 through 8
- IN-OFFICE
- Hart chart rock
- Bug on string
- Loose lens rock ; add minus lenses
- Tranaglyphs or vectograms : base-in
- Use even more detailed targets such as tranaglyph Sports Slide and Faces targets and the Spirangle vectogram
- Computer Orthoptics Random Dot program: base-in
- HOME THERAPY
- HTS accommodation program
- Hart chart rock
- HTS Vergence program
- Phase 2
- Sessions 9 and 10
- IN-OFFICE
- Loose lens rock; use both plus and minus lenses and incorporate speed as a factor
- Tranaglyphs or vectograms with modifications to create jump vergence demand: base-in
- Nonvariable tranaglyphs
- Tranaglyph 515 or the Quoit vectogram: base-out
- Binocular accommodative therapy techniques: use any of the binocular techniques listed above with ± lenses.








{kind=link}