
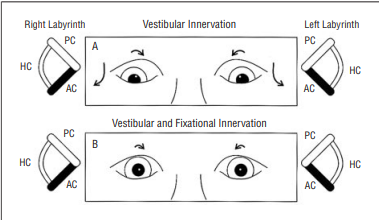
A bilateral lesion that injures both anterior canal pathways or disinhibits both posterior canal pathways will increase prenuclear innervation to the superior oblique and inferior rectus subnuclei, resulting in a posterior canal predominance and increased downward tonus to both eyes. This downward tonus must be overcome by fixational innervations.
Since the inferior rectus muscles retain their vertical field of action in adduction while the superior oblique muscles have minimal vertical action in abduction, this downgaze predominance would produce a relative overdepression of the adducting eye in lateral gaze.
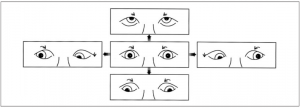
Activation of both superior oblique muscles produces bilateral intorsion in the primary position and an A pattern due to the tertiary abducting action of the superior oblique muscles in downgaze. In addition, binocular intorsion rotates the inferior rectus insertions laterally and reduces the adducting action of the inferior rectus muscles in downgaze.
The vestibuloocular pathways pass through the posterior fossa and are susceptible to injury when structural abnormalities involve the brainstem or the cerebellum. In children with hydrocephalus and myelomeningocele, the constellation of A-pattern strabismus, bilateral superior oblique muscle overaction, and bilateral intorsion is often associated with tonic downgaze early in life.29-38 Children with myelomeningocele not only have hydrocephalus but also frequently have an associated Chiari II malformation.35,36 Since prenuclear input to the vestibular system from the vestibulocerebellum is primarily inhibitory, bilateral compression of or injury to those vestibulocerebellar pathways activating the anterior canals would disinhibit the posterior canals and increase extraocular muscle tonus in their target muscles.
Previous investigators35-40 have speculated that bilateral superior oblique muscle overaction may be supranuclear or prenuclear in nature, citing the frequency with which it accompanies defective upgaze. Biglan37,38 attributed the overacting superior oblique muscles, A pattern, and chronic downward deviations of the eyes in children with myelomeningocele to defects in the vertical gaze pathways producing either a failure to inhibit the downgaze pathways or excessive stimulation of downward gaze. Acute comitant esotropia caused by neurologic disease such as hydrocephalus or Chiari malformation is often associated with bilateral superior oblique muscle over action.39 Although orbital anatomical factors have also been implicated as a cause of superior oblique muscle overaction in hydrocephalus,1,29 the high frequency of structural abnormalities within the posterior fossa led Hamed35,36 and colleagues to propose that superior oblique muscle overaction and alternating skew deviation in lateral gaze may share a common neuroanatomical substrate. Recently, Hoyt41 has observed that premature infants with periventricular leukomalacia or intraventricular hemorrhage may Initially manifest a tonic downgaze that evolves into an A-pattern esotropia and bilateral superior oblique muscle overaction.









{kind=link}