
Accommodation Paralysis after Pheniramine Maleate Injection:
Partial third nerve palsy
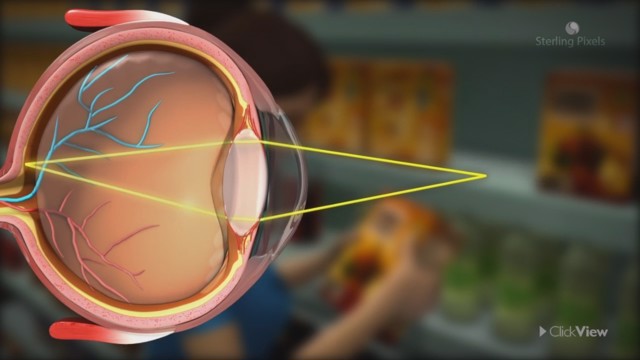
Cycloplegia (accommodation paralysis) causes blur for near as well as distance in the far-sighted child.
effects of drugs as well as various systemic, neurological, and local ocular pathologies can cause accommodative insufficiency and loss of accommodation. A 29-year-old man was admitted to an ophthalmology department with blurred vision and diagnosed as suffering from acute accommodation paralysis. He had a history of being given a pheniramine maleate injection for pruritus 20 days previously. Symptoms began immediately following the injection. After systemic evaluation and laboratory tests, he was diagnosed as having Gilbert syndrome. His complaints and symptoms recovered in approximately a further 10 days. Metabolism of pheniramine maleate can be impaired in Gilbert syndrome and anticholinergic effects can cause accommodation paralysis.
Introduction
Loss of accommodation is a normal process of ageing, called presbyopia. However, premature or acute accommodation loss in a child or young adult necessitates systemic evaluation and laboratory work-up to determine the aetiology. The most common cause of acute loss of accommodation is an unwanted drug effect. Therefore, a detailed medical history and systemic evaluation should be carried out in every patient with acute loss of accommodation.1 A case of accommodation paralysis following antihistaminic drug injection is described in this case report.
Case Report
A 29-year-old man was admitted to
Department of Ophthalmology with blurred vision for the previous 20 days. The patient had undergone a complete ophthalmic examination. Uncorrected visual acuities for distance were 3/10 in the right eye and 4/10 in the left eye; best corrected visual acuities were 7/10 in the right eye and 8/10 in the left eye. Slit-lamp biomicroscopy and dilated fundus examinations were normal. Intraocular pressures were 16 mm Hg. There was a reduced pupillary response to light and near bilaterally. His manifest refraction without cycloplegia was +0.75 D and dynamic retinoscopy for near was also +0.75 D bilaterally. Retinoscopy revealed a refractive error of +1.0 bilaterally after cycloplegia. There was no visual field defect, his optical coherence tomography of the retina was within normal limits in each eye.
The patient’s medical and family history was unremarkable. He had a history of drug use on one occasion about 20 days previously. He had been admitted to an emergency department with the complaining of pruritis. Pheniramine maleate had been injected intravenously. Just after the injection he had noticed blurred vision. There were no other symptoms except slight buccal dryness.
The patient was seen by the internal medicine department for systemic evaluation and laboratory tests were done. Unconjugated hyperbilirubinaemia was found; other liver function tests were normal. He was diagnosed as Gilbert syndrome. He did not have any complaints related to this disease previously.
At the second visit, 4 days after the initial examination, the patient’s symptoms had worsened. Uncorrected visual acuities were 2/10 in both eyes. Best corrected visual acuities were 5/10 (right eye) and 4/10 (left eye) with hyperopic correction; he was unable to read and see at near. Pilocarpine (2%, 2×1) was prescribed, but the patient did not report any improvement.
One week later, the symptoms began to recover and his uncorrected visual acuities were 10/10 in both eyes. Noncycloplegic retinoscopy for distance was +0.50 D and dynamic retinoscopy for near was −1.50 D for both eyes. Pupillary function returned to normal as his vision recovered.
At 1-month follow-up his ophthalmological examination was normal.
Although loss of accommodation is a normal ageing process, accommodative insufficiency or acute accommodation loss in a child or young adult can be seen and cause blurred vision, asthenopia, and headache.2,3 Systemic, neurological, and local ocular pathologies can cause accommodative insufficiency. Head trauma, Parkinson disease, multiple sclerosis, encephalopathies, meningitis, midbrain pathology, subdural haematoma, pharmacological and toxic agents, viral infections, diabetes, botulism, diphtheria, and oculomotor nerve palsy are among causes of accommodation insufficiency.4,5 Exposure to systemic anticholinergic agents can also cause acute accommodative loss.6
According to their sedative side effects, histamine H1 receptor antagonists are classified as first-generation and newer-generation antihistamines.7 Pheniramine maleate is an alkylamine derivative of first-generation antihistamines. First-generation antihistamines are less selective and they have more side effects than newer-generation antihistamines. At higher doses and concentrations, their selectivity decrease and cholinergic, serotonergic, and catecholaminergic systems can be effected. They can inhibit muscarinic receptors competitively.8 As a result of the anticholinergic effect, blurred vision, tachycardia, urinary retention, and constipation can be seen.9 Pheniramine maleate is metabolised by hepatic hydroxylation, demethylation, and glucuronidation. Glucuronidation consists of transferring the glucuronic acid component of uridine diphosphate (UDP) glucuronic acid to a substrate utilising the UDP glucuronosyltransferase enzyme. Gilbert syndrome is a common, mild liver condition characterised by reduced UDP glucuronosyltransferase enzyme capacity, in which the liver does not properly process bilirubin produced by the breakdown of red blood cells. Gilbert syndrome (pronounced: zheel-BAYR as Gilbert was French) is caused by an inherited gene mutation, is typically harmless, and does not require treatment. Patients born with Gilbert syndrome can stay undiscovered for many years and it is often discovered by chance, mostly with a routine blood test showing elevated bilirubin levels. It is also known as constitutional hepatic dysfunction or familial non-haemolytic jaundice. However, blood concentration of drugs metabolised by this enzyme can increase in patients with Gilbert syndrome and this can cause adverse effects, as seen in our patient.
To the best of our knowledge, our case is the first reported case of accommodation paralysis after pheniramine maleate injection due to reduced UDP glucuronosyltransferase enzyme capacity in Gilbert syndrome. As a consequence of reduced pheniramine maleate metabolism, anticholinergic side effects can cause accommodation paralysis as in our patient who was admitted initially with ocular complaints and diagnosed as Gilbert syndrome following systemic evaluation. He only had slight dry mouth as another symptom of anticholinergic toxicity. In addition to the loss of accommodation affecting near vision, the patient was also hyperopic, which, with peripheral aberrations associated with pupillary dilatation, resulted in a decrease in distance acuity. Patients with Gilbert syndrome should be warned about possible side effects of the drugs that are metabolised in liver and they should be aware of the need to inform their physicians of this otherwise benign condition.







{kind=link}