
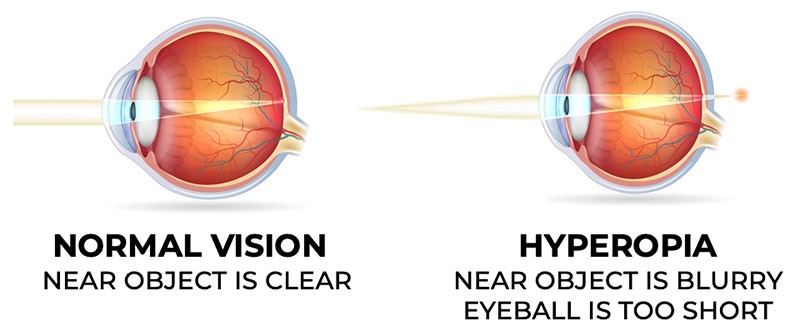
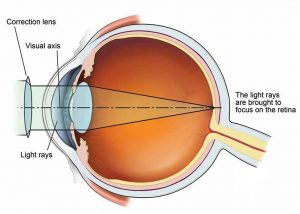
The term of high hyperopia first was suggested by Kastner in 1775. The term high hyperopia means “excess measure of the eye”. The term hyper means in excess met means meaure and opia means eye. The high hyperopia or hypermetropia is the refractive error of the eye wherein the parallel rays of light coming from infinity are focused behind the retina.
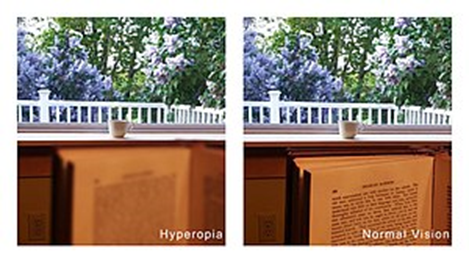
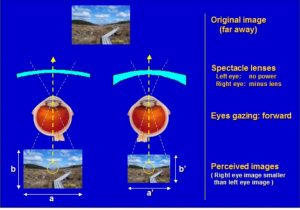
In high hyperopia rays coming from a point will be divergent than the rays of emmetropic eyes. So high hyperiopia eyes creat blurred image and a clear image is impossible. Clear image is only possible when converging power is increased that by a convex lens.
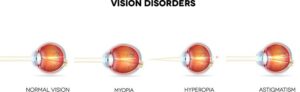
Hyperopia may also be categorized by the degree of refractive error. Low hyperopia is +2.00D or less, moderator hyperopia ranges from +2.25 to +5.00D, and high hyperopia +5.25D or more. High hyperopia may be associated with blurring of the optic disk margin, known pseudopapilledma.
□ SYMPTOMS: In high hyperopiac patients symptoms very depending the person age group but few symptoms are group but few symptoms are commonly seen. These can be grouped as bellow:
ASYMPTOMATIC: It is mainly occurs young patients those refractive error is less than +1D. It is usually corrected by mild effort of accommodation without production any symptom so patient cannot his/her refractive error.
ASTHENOPIC SYMPTOMS: It occurs [+1-(+2)] D high hyperopia is fully corrected by effort of accommodation and sustained asthenopic symptoms. These include:
Tiredness of Eye.

Headache. Mild Photophobia.

These symptoms progress as day by day and are aggravated by prolonged use of near vision.
The are some children with high hyperoia who are intolerant of spectacles or contact lenses but who appear to benefit significantly from surgical refractive correction, according to Ken Nischal FRCOphth, Children Hospital, University of Pittsburg, US.
“We know that hyperopia will not only cause amblypia but will also have a behavioural effect if it’s left uncorrected. Nonsurgical management of high hyperopia is very successful in the majority of children. However, there is a miniority of children who don’t copy with convergental therapies and they are the ones we hope to help with refractive surgery,” Dr. Nischal said at the XXXI congress of the ESCRS in Amsterdam.
Studies have shown that, without correction, there is a high risk of amblyopia in cases where there is more than 4.0 D of bilateral hyperopia, anismetropic hyperopia of greater than 1 D or hyperopic astigmatism of greater than 1.5 D.
Moreover, high hyperpia can have permanently damaging consequences for a child’s fine motor skills and education. There is a great volume of published rescharch showing that children with hyperopia of greater than 4D tend to have a lower level of educational achievement at primary school level.
BLUURED VISION WITH ASTHENOOIC SYMPTOMS: In amount of refrective error[+2 to +4] D that cannot be corrected by the effort of accommodation but due to sustained accommodative efforts patients develops asthenpoic symptoms, then the patient complains of detective vision more for near than distance associated with asthenopic symptoms.

CONVERGENT SQUINTS: In high amount of hypermetropia cannot by the by the effort of accommodation but young patients tired to effort of accommodation but young patient tried to effort of accommodation, occurs excess of convergence and muscle dissociation that produces convergent squints.
EARLY PRESBYOPIA: When amount the high hyperopia(>4D) is more, the patients usually do not accommodation(adults patients) and occurs defective vision for near and distance.

PSEUDOMYOPIA: Spasm of cilliary muscle induce pseudomyopia. Pseudomyopia can be detected by cyclopegic refraction.
AMBLYOPIA: Ambyopia by definition refers to patients reversible loss of vision in one or both eyes. It develop in some cases.
- STABISMIC AMBLYOPIA: Occurs in children with developing accommodation convergent squint.
- ANISOMETROPIC AMBLYOPIA: When the one eye having higher degree of refrective error than the other eye. It mainly occurs unilateral hypermetropia.
- ISOAMETROPIC AMBLYOPA: It is bilateral hypermetropia occurs in children with bilateral uncorrected high refractive error
PRIMARY ANGEL CLOSURE GLAUCOMA: The eye in high hyperopia is small with a comparatively shallow anterior. Due to regular in size of the lens with increasing age, these eye become prone to angle closure disease.
DIPLOPIA: Diplopia refres to simultaneous perception of the two images of a single image. Diplopia may be binocular. In high hyperopia binocular uncrossed diplopia may be seen.
UNCROSSED BINOCULAR DIPLOPIA: In uncrossed diplopia the flase image is on the same side as deviation. It occurs in convergent squint as in lateral rectus paralysis.
IN HIGH HYPEROPIA IS NOT CPRRECTED FOR A LONG TIME. THE FOLLOWING SYMPTOMS MAY OCCUR:
Stye.
Blepharitis
Chalazian
SIGN:
SMALL EYE BALL: The eyes are small or normal the occurs in microopthalmos and nanoopthalmos.

SMALL CORNEA: Cornea may be slightly than the normal. There can be cornea plana.
LENGTH OF EYE BALL: In high hyperopia the anteroposterior of length of eye ball is very small.
SHALLOW ANTERIOR CHAMBER: In high hyperopia eyes also seen shallow anterior chamber.
FUNDUS:
OPTIC DISC: Optic disc which may look small and reddish in colour with ill- defined margins and even stimulate papillities, there is no swelling of the disc so it called pseudo papillites.
MACULA: Foveal reflects may be situated at greater distance from the optic disc margin.

GENERAL BACKGROUND: The retina as a whole may shine due to greater brilliance of light reflections. It is called shot silk retina.
RETINA VESSELS: Retina vessels reflexes may be accentuated. The vessels may show undue tortuosity or abnormal branching.






{kind=link}