
Ammetrpia ?
Contact lens ?
How to manage ammetrpia with contact lens ?
How to wear contact lens ?
When you avoid contact lens and when is better to wear contact lens ?
If you interested to read this blog . I will discuss on this topic may be it will be helpful for you . Here the topic denoted as correction of ammetropia with contact lenses.
If you read it with deep concentration, you achieve an amazing knowledge. You will be very glad after knowing this fact.
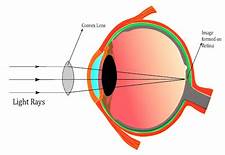
So, let us move on the topic.The topic is Ammetropia correction with contact lens. At first, we should take a short idea that what Ammetropia. There are two conditions of eye, good eye that means there are no any type of problem(here I indicate specially refractive error), and the other thing is, there are may be some problems(here I indicate again refractive error that condition is called Ammetropia. So, we understand that ––– Ammetropia means abnormality in refractive error, there are some problems in refractive media as a result. Who has Ammetropia, he may be suffers from short sightedness, long sightedness, short and long both sightended; and the other type of problem is, they are not able to see image, letter or object distinctly and clearly. All the condition under goes to to the Ammetropia condition. So we noticed that there are various types of problem, occurs — (1) Short sightedness (2) Long sightedness (3) and the other type is Astigmatism. Now I enter into the topic Short sightedness (myopia) At first, we should take an idea about Myopia. Myopia Myopia is a type of refractive error when the parallel light rays are coming from infinity and after passing the refractive media (Cornea→Aqueous humor→Crystalline lens→Vitreous humor) the light rays are focused in front of retina, when accommodation is being rest this condition is called Myopia.
If a person have – 4.50 DS power in spectacle , then the patient is interested to wear contact lens then there power will be -3.25 DS in generally .
Now we discuss about Long Sightedness(Hypermetropia)
~At first, we should know about Hypermetropia.
~What is Hypermetropia?
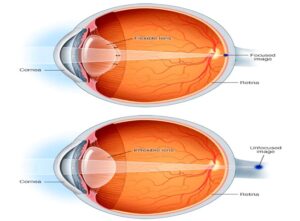
Hypermetropia → When the parallel light rays are coming from infinity and after passing the refrective media (Cornea→Aqueous humour→Lens→Vitreous humour) and focus behind the retina, when accommodation is being rest, this condition is called Hypermetropia.
In generally, Hypermetropia correction convex (➕) lens. Here we discuss the difference between the spectacle correction and the contact lens correction.
If a patient have +5.50 DS power in spectacle , then the power of contact lens will be +5.75 DS in generally.
Now we are going to an interesting topic ––
The topic is Astigmatism.
At first, we should know what is Astigmatism.
When the two parallel rays are passing through the cornea–crystalline lens, they are not focused in a single point instead of it form a focal line, this condition is called Astigmatism.
Astigmatism is mainly two types——
(1) Regular Astigmatism
(2) Irregular Astigmatism.
Astigmatism error correction with spectacle and contact lens. But there are much advantage to use the contact lens for Irregular Astigmatism.
If the patient have – 2.00 DS / + 0.50 DC * 180 then the contact lens power will be – 2.25 DS. If the patient have – 7.00 DS / -1.50 DC * 90 , then contact lens power will be – 7.75 DS / – 0.75 DC * 90.
Now we will take a short idea about contact lens , Here contact indicate that directly contact with the cornea and which basically made with thin plastic , so we say to that Contact lens is a thin plastic lens placed directly on the surface of the eye to correct the visual field ( refractive error ).
There is a wealth of research information to show that specific types of contact lenses are the best way to both correct your child’s vision and slow the progression, or worsening of myopia (shortsightedness). If you are interested in evidence based myopia management for your child, the discussion with your optometrist will most likely include contact lenses. While some children will never be willing or suitable to wear contact lenses, for various reasons, the truth of the matter is most kids can wear contact lenses safely, happily and successfully. Here’s the science.
Firstly, there appears to be no additional risk of adverse events (eye inflammations and infections) when commencing contact lens wear as a child (aged 8–12 years) compared to as a teenager. A study evaluating outcomes after ten years of contact lens wear in people who started wearing contact lenses as either kids or teens found no difference between these groups.
Secondly, the risk of an eye infection (the type us optometrists are most concerned about is a corneal ulcer, called ‘microbial keratitis’) is very low in the types of contact lenses optometrist typically fit to kids. The safest way to wear contact lenses are daily disposable lenses, which carry a risk of 2 events per 10,000 patient wearing years. This means that if your child wears contact lenses for 10,000 years (which she probably wont!), she will be at average statistical risk of two eye infections. Low odds, correct? There are two types of daily disposable lenses available across the world for myopia management — Coopervision’s MiSight and Visioneering Technologies NaturalVue — but your eye care practitioner’s access to the lenses varies depending on what country you’re in.
If your child wears reusable soft contact lenses — in myopia management these are ‘multifocal’ contact lenses — these lenses are worn each day and then cleaned, stored overnight and kept usually for a month. The risk of infection increases with these, because of the extra bits and pieces involved (the storage case and solution), and not getting a fresh lens every day as you do with daily disposables. So the risk of infection with these lenses is 12 per 10,000 patient wearing years. Eeek, this is six times higher than daily disposables?? Yes, but the risk is still 1 eye infection for every 1,000 years your child wears contact lenses. He probably won’t wear them that long, either! Most optometrists have access to some type of multifocal contact lens, suitable for myopic children.
If your child wears overnight orthokeratology — lenses which gently reshape the surface of the cornea so no glasses or contact lenses are required during the day — the risk is similar to the multifocal lenses, at 13 per 10,000 patient wearing years. This is a similar risk to reusable soft contact lenses, as described above.
What’s the riskiest way to wear contact lenses? Overnight wear of soft contact lenses, which carries double the risk of multifocal or overnight orthokeratology lenses, of 25 per 10,000 patient wearing years. Rarely would children be fit in this way, unless there are special circumstances.
Converging Contact Lens for Hyperopia: In far-sightedness (hyperopia), the natural lens of the eyes has a decreased potential to refract light emitted by an object, thereby making the focus at a location beyond the retinal layer. The contact lens that is convex or converging in nature is used to correct this condition.
Toric contact lenses are often the best choice for contact lens wearers with an astigmatism, because they’re specifically designed to address the problem. The special shape of a toric lens creates different refractive, or focusing, powers that can help correct either a corneal or a lenticular astigmatism.
Can you wear regular contact lenses if you have astigmatism? A: No, if you have astigmatism, it’s essential that you wear specialized contact lenses because your condition can worsen if not. Regular contact lenses do not cover your cornea’s entirety, which will impair your ability to see even further.
Power selection manifest refraction with a vertex distance conversion . convert the plus cylinder Rx into minus cylinder. (Transposition) .convert the patient’s refraction to spherical equivalent (SE) . For AST correction may need a a toric lens.
Cylinder Prescription Protocol for Scls 1)If cylinder in refraction is ≤ 0.50D, CL power = spherical component 2)If cylinder in refraction is 0.750D to 1.00D, CL power = SE (spherical component + 1/ 2 Cyl) 3)If overall spherical component in 1 and 2 is >± 4.00 D, compensate for vertex distance using either method 1 or 2.
Power selection/ Vertex Distance .Method 1, Fc = Fs / 1- d Fs . Fc = power of CL, Fs = power of spectacle lens, d = distance between spectacle lens and CL in meter .Method 2 , Add 1/2 of cyl to sphere + (calculation table) EX: Ref; -5.00 +1.00 x 90 (plus cyl form) -4.00 -1.00 x 180 (minus cyl form) vertex distance = 13mm = 0.013m Fc = 4.5 / 1- (0.013 x 4.5) Fc= 4.5 / 0.9415 = 4.249 ≈ 4.25D or contact lens power = – 4 + – 0.50 = – 4.50D The contact lens power from the table = – 4.25D.
Fit evaluation Allow the CL to rest on the eye for 5 minutes before evaluating the fit. Lens centeration, after each blink Lens movement. PUSH UP TEST Lens Coverage- limbus to limbus No movement, the lens is too tight. Much movement, the lens is too loose. The VA should be stable and remain so before, during, and after each blink. If the VA is not as clear as expected, do an over- refraction and check for residual astigmatism. Dryness can cause fluctuating VA or decreased VA.
Signs and symptoms of a steep fitting lens Fluctuating VA, clears after each blink Comfortable at first, then not Circum corneal injection .Circum corneal indentation. Conjuctival drag .Vessel blanching.Little or no movement upon each blink . Keratometry mires distorted, then clear after each blink . Air bubbles centrally, over pupil.
Signs and symptoms of a loose (flat) fit .VA unstable with each blink . Patient awareness of the lens . Poor centering, especially low fitting .Too much movement with each blink .Edge “stand off” (edges do not hug the eye) .Lens falls out .Air bubble under the lens, especially on the periphery of the lens .“K” mires are blurred after each blink.
Modifications Correcting a FLAT fit Correcting a STEEP fit.Tighten/decrease the base curve but keep the diameter the same. Increase the diameter and keep the base curve the same. Loosen/increase the base curve, but keep the diameter the same. Decrease the diameter and keep the base curve the same.
Holding your eyelids openwith the index finger and thumb of your non-dominant hand, look straight ahead and place the lens over your eye. try to blink your eyes a few times to help the lens set into position correctly. Give the lenses a few minutes to naturally settle into the correct orientation on your eyes.
Your eye care practitioner will be the best guide of which option is most suitable for your child, as it can depend on their level of myopia, eye shape and more. It can depend on in which country you live as to which options your eye care practitioner has available. It is also important for your eye care practitioner to understand which will suit you, your child and your family better.








{kind=link}