

WHAT IS SQUINT?
= A misalignment of the visual axes of the two eyes is called squint or strabismus .
Classification of strabismus :
1)Latent squint:-it is a condition in which the tendency of the two eyes to deviate.
it has four types- esophoria, exophoria, hyperphoria, cyclophoria.
2)manifest squint
What is manifest squint ?
The constant or intermittent deviation of the visual axis of one eye from the point of fixation, which is seen with both eyes open.
It is two types:-
Concomitant squint
Incomitant squint
Concomitant squint:-
When the amount of deviation in the squinting eye remains constant in all the directions of gaze, and there is no limitions of ocular movements this type of manifest squint is called concomitant squint.
Clinical features of concomitant squint:-
- Ocular deviatiation( unilateral or alternate deviation, inward or outward deviation or vertical squint)
- Refractive errors
- Suppression or Amblyopia.
Types of concomitant squint
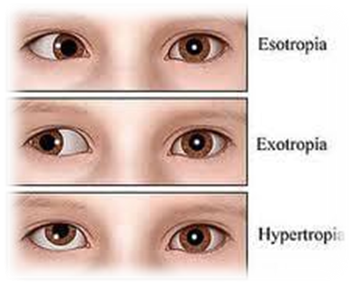
- Convergent squint it’s called esotropia
- Divergent squint it’s called exotropia.
- Vertical squint it’s called hypertropia.
Convergent squint:-
Concomitant convergent squint or esotropia means inward deviation of one eye. it can be unilateral or alternating.
Classification of concomitant covergent squint:-
- Infantile esotropia
- Accomodative eaotropia
- Acquired Non accommodative esotropia
- Sensory esotropia
- Consecutive esotropia
Infantile esotropia :- It is called as congenital esotropia. It is usually occurs at 2-4 months of age. Amblyopia develops in 25-40 % of cases due to prefers to fix with one eye.
Accommodative esotropia:- It occurs due to overaction of convergence associated with accommodation reflex. Accommodative esotropia is the most common type of squint in children. It develops around 2-3 years of age. It is mostly accommodative.
It has three types.
- Refractive accommodative esotropia
- Non-refractive accommodative esotropia
- Mixed accommodative esotropia.
Refractive accommodative esotropia:- It is caused by a normal AC/A( Accommodative convergence/Accommodation) ratio.it usually develops at the age of 2-3 years of age.
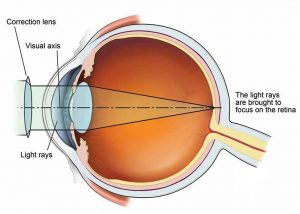
Treatment:- it is fully corrected with a convex lens.
Non-refractive accommodative esotropia:- It is caused abnormal large AC/A ratio. It usually occurs in patients who have no refractive errors.
Treatment:- it usually corrected bifocal glass with add+3DS.
Mixed accommodative esotropia:- It is caused by hypermetropia and a high AC/A ratio.
Acquired non-accommodative esotropia.
Sensory Esotropia:- during cataract, severe congenital ptosis, aphakia, anisometropia, optic atrophy, retinoblastoma, and so on diseases that prevent the development of normal binocular vision or interfere with its maintenance.
Consecutive esotropia:- when surgical overcorrect of exotropia.
Divergent squint:- Concomitant divergent squint or exotropia means outward movements of one eye, when the one eye is fixed.
Classification:-
Congenital exotropia:- it is usually seen <6 months of age. But it is rarely seen at birth. It is characterized by a fairly large and constant angle of squint, usually alternating with homonymous fixation in lateral gaze.
primary exotropia;- it may be unilateral or alternating and may present as intermittent or constant squint.
sensory exotropia:- in traumatic cataract, corneal opacity, optic atrophy, amblyopia, retinal detachment exotropia developed.
consecutive exotropia, surgical overcorrection of exotropia that occurs consecutive exotropia.
Incomitant strabismus
It is a type of heterotopia in which the amount varies of deviation varies in different directions of gaze.
- Paralytic squint
- ‘A’ and ‘V’ pattern
- Restrictive squint
Paralytic squint:- it refers to ocular deviation resulting from complete or incomplete paralysis of one or more extraocular muscles.
Neurogenic lesions:- it occurs absences of 3rd and 6th cranial nerve palsies, birth injuries, encephalitis, meningitis, neurosyphilis, peripheral neuritis, brain tumors, hypertension, diabetes mellitus, artheoscelorosis, diphtheria toxins and diffuse sclerosis
Myogenic lesions:- hypoplasia, weakness, and musculofacial anomalies, laceration, dissertation, influenza, measles, bilateral ptosis, diplopia.
Neuromuscular junction lesion:- it includes myastenia gravis.
Clinical features:-
Sign:- diplopia, amblyopia, confusion, nausea, vertigo.
‘A’ and ‘V’ pattern hetertopia:- It produces when squinting eyes varies more than 10 PD and 15 PD with other eyes, Respectively between upward and downward gaze.
Restrictive strabismus:- The extraocular muscles are not paralyzed but the movement is restricted.
Test for detect manifest strabismus:-
Direct cover test,
Alternate cover test
Hisberg corneal reflex test
The prism and cover test,
Modifies krimskey corneal reflex test.






{kind=link}