
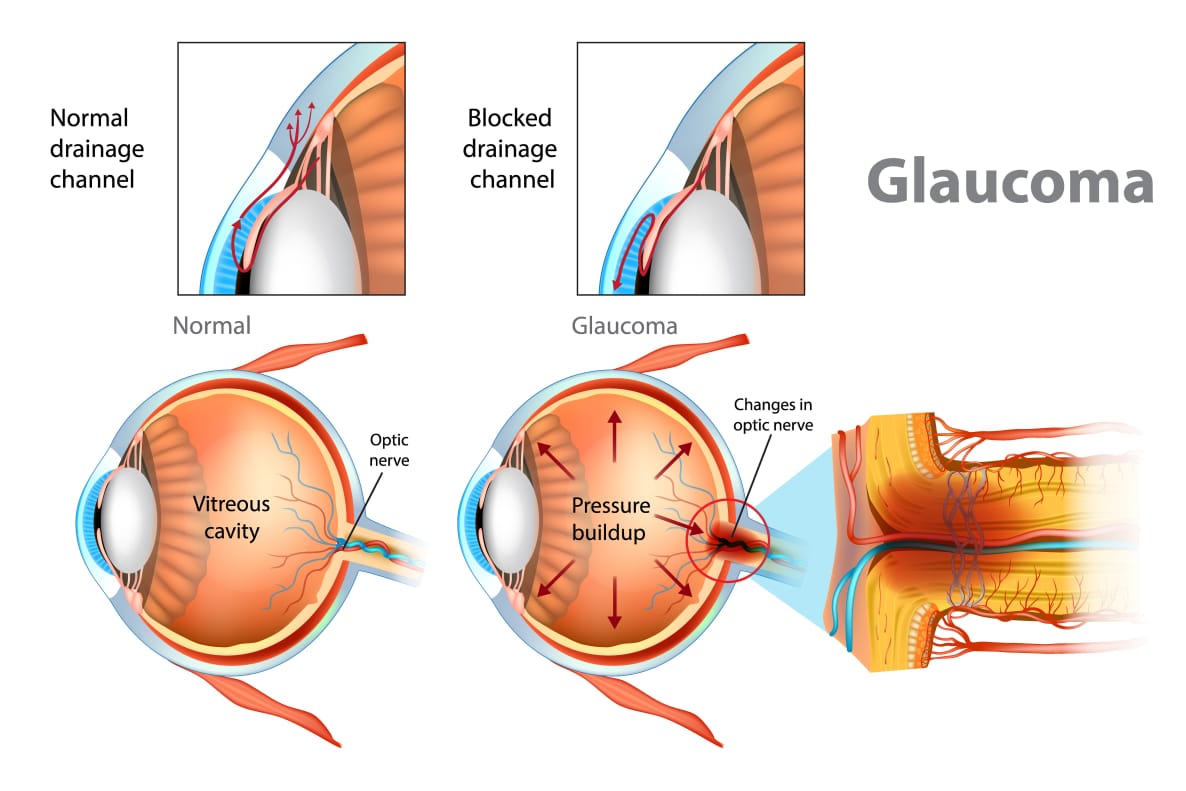
CONGENITAL OR INFANTILE GLAUCOMA:-
Medications are not very effective and so treatment of congenital glaucoma is primary surgical. However, IOP must be lowered by medical treatment with hyperosmotic agents, carbonic anhydrase inhibitors and beta-blockers(timolol 0.5% is the first drug of choice) till surgery is taken up.
•Miotics are not used in such cases because they paradoxically increase IOP.
•Alpha-2 agonist causes CNS depression in children and is thus contraindicated.
SURGICAL PROCEDURES for congenital glaucoma:-
1.Incisional angle surgery, which can be performed by the internal approach (goniotomy) or by external approach (trabeculectomy).
i) GONIOTOMY-In this procedure, a barkan’s goniotomy knife is passed through the limbus on the temporal side. Under gonioscopic control the knife is passed across the anterior chamber to the nasal part of the angle. An incision ia made in the angle approximately midway between root of the iris and schwalbe’s ring through approximately 75°.The knife is then withdrawn. Although the procedure may have to be repeated, the eventual success rate is about 85%.
ii) TRABECULECTOMY-This is useful when corneal cloding prevents visualization of the angle or in cases where goniotomy has failed. In this, canal of schlemm is exposed at about 12 o’ clock position by a vertical scleral incision after making a conjuntival flap and partial thickness scleral flap. The lower prong of harm’s trabeculectomy is passed along the schlemm’s canal on one side and the upper prong is used as a guide. Then the trabeculectomy is rotated so as to break the inner wall over one quarter of the canal. This is, then repeated on the other side. The main difficulty in this operation is localization of the schlemm’s canal.
2.Filteration surgery is required in many cases.
a. Trabeculectomy with antimetabolites gives good result.
b. Combined trabeculectomy and trabeculectomy with antimetabolites has been accepted as the standard procedure.
3.Glaucoma drainage devices(GDD) are required in incalcitrant cases.
PRIMARY ANGLE-ClOSURE GLAUCOMA:-
In early stages (intermittent attacks)
•MIOTIC THERAPY: Instillation of pilocarpine 2% every 5 minutes, is usually effective in pulling the inis from the angle and aborating the attack .The fellow eye in should be treated with 2%. pilocarpine, 3 times daily.
•Yttrium aluminum garnet loser peripheral imidotomy (YAG PI) or surgical peripheral iridectomy (Surgical PI) should then be performed in both eyes.
In acute congestive attack: Although ,the treatment of acute PACG IS essentially surgical, the initial treatment is medical.
MEDICAL THERAPY:
•Tablet · acetazolamide (250mg) : 2 tabs stat, and then followed by 1 tablet 4 times daily, with potassium supplement.
•Hyperosmotic agents: They act by drawing water out of the eye and reduce the IOP
_Intravascular injection of mannitol (20%.):
dose is 1-2 g/kg body weight, i.e 300-500 mL is given intravenously over a period of 30-45 minutes.
– Oral glycerol (50%. solution): 30mL of punc glycerol with equal amount or fruit juice Stat, and then 3 times daily. cannot be used in diabeties.
Isosorbide: It is used orally ,and it does not cause nausea. It can be used safely in diabetic patients.
• pilocarpine (2%. Or 4%) eye drop is instilled every 5 minutes till the pupil gets constricted then 3-4 times daily. The fellow eye be treated simultaneously with pilocarpine 2%. 3 times daily.
•Strong analgesies and antiemetic may be needed to reduce pain and vomiting.
•Steroid – antibiotic drops are instilled frequently to reduse congestion. Once the IOP has been reduce medically and eye becomes quiet, the further management is
_continue medical treatment with pilocarpine 2%. crrop. 3- 4 times daily. This is only indicated in old patient with poor general health, and where a laser is not available.
•SURGERY
i) Laser iridotomy or surgical peripheral iridectomy and if necessary
ii) Filtration surgery
•Surgical therapy: A careful gonioscopy is necessary in deciding the percentage of angle closere by peripheral anterior synechiae, before considering the therapy of surgery.
_If the angle -closure is less then 50% then laser iridotomy or a surgical peripheral iridectomy should suffice.
_If the angle-closure is more than 50% then a filtration operation in indicated.
PRIMARY OPEN-ANGLE GLAUCOMA:-
MEDICAL THERAPY:
The treatment of POAG is in the first place, with operation as a last resort.
1. Beta-blockers :
Timolol maleate, betaxolol and levobunolal
– Timolol maleate (0.25% or 0.50%) eye drops at 12 hourly interval(twice daily) -Betoxolol (0.5%) eye drops twice daily. •It is candioselective Beta 1 blocker and is almost as effective as timolol.
•It has little effects on cardiopulmonary system, and may be used safety in bronchial asthma.
-Levobunolol (0.5%) eye drops twice
daily. It is as effective as timolol with lesser ocular side effects.
2. Prostaglandin analogs (PGAS) prostaglandin analogs CPGAS) act by increasing the uveoscleral outflow by over 100% of physiological levels. It lowers IOP by 25-35% from baseline.The once daily dosing and minimal ocular side effects advantageous . But there are expensive drugs
•Latanoprost (0.005% ) eye drop
•Travoprost (0.004%.) eye drop •Bimatoprost (0.003% or 0.01%) eye drop
•Tafloprost (0.0015%) eye drop
3.ALPHA AGONISTS
-Brimonidine tartarate Co.1%, 0.15%. or 0.2%) eye drop . Recommended dose is two times daily. Brimonidine has a dual mechanism of action
-(i) by reducing aquous production
-(ii) Increasing uveoseleral aqueous outflow.
– It may cause fatigue and or drowsiness in some patients.
– Epinephrine (0.5%., 1%. or 2%.) eye drops twice daily and is useful in young patients,.It is a nonspecific adrenergic agonist.
4. TOPICAL CARBONIC ANHYDRASE INHIBITORS (CAIS)
-Dorzolamide (2%) and brinzolomide (1%) ophthalmic solution, 3 time daily They IOP by reducing aqueous production.Most significant side effect is on corneal endothelium.
5. Mioties pilocarpine nitrate (1%,2%. or 4%) eye drop 3-4 times daily. 2%. solution is commonly used.
LASER THERAPY:-
Argon Casen trabeculoplasty (ALT) is indicted when POAG is not well controlled with medical therapy.
● Mechanism:Burn in the trabecular meshwork for 360° by argon laser→ shrinkage and fibrosis of collagen opening up of intertrabecular spaces →increase in aquous outflow. It works better in whites than amkng blacks .
It is safe noninvasive opp procedure.The average drop in IOP is 8-10 mm. Hg.
SURGICAL THERAPY:-
The indications for surgical theraphy are
•POAG cannot be controlled with maximal medical therapy.
•The patient cannot tolerate medical treatment due to toxicity.
•The compliance of the patient is por or when the follow-up is unreliable.
•Some surgeons prefer early surgical intervention.







{kind=link}