
Hyperopia or hypermetropia is very common in children and adults. The progression of hyperopia gradually decreases by increasing the age of a child. Compared to children the adult hyperopic patients have to go to their near by optometrist for assessment of vision regularly.
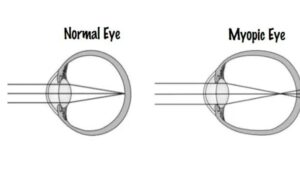
Clinically the definition of hypermetropia is ” Hypermetropia is a type of Refractive error of the eye where parallel Ray’s of light coming from the infinity are focused behind the light sensitive layer of retina, accommodation being at rest.
A hyperopic patient spontaneously uses his/her accommodative effort, crystalline lens’s converging power to overcome the circumstances. By birth most human beings are hyperopic. The size of the eyeball increases with the progression of age, then the eye may become emmetropic or even myopic.
Hereditary role : The family history plays a important role in hyperopic patients. Nanophthalmos is a rare inherited disorder characterized by extreme axial hyperopia. Membrane type Frizzled Related Protein (MFRP)
gene is responsible for this.
Clinical Types of Hypermetropia :
Generally the clinical types of hyperopia is
i) Simple hyperopia
ii) Pathological hyperopia
iii) Functional hyperopia
Simple hyperopia
It is very common type. It includes axial and curvatural due to biological variations in the development of the eye. It may be inherited.
• Axial hyperopia : Axial hyperopia is very common. In this condition the total Refractive power of eye is normal, but there is axial shortening of eyeball ( 1 mm shortening of eyeball = 3 Dioptres ( D) of hyperopia.
• Curvatural hyperopia : In this condition curvature of the cornea becomes flatter than the normal, resulting in change in Refractive power of the eye. About 1 mm increase in radius of curvature results in 6 D of hypermetropia.
Pathological hyperopia
Pathological hyperopia occurs due to congenital or acquired. In pathological type anomalies lie outside the limits of biological variations. It can be.
● Acquired hypermetropia : It is seen in old age due to
• Curvatural hyperopia There is decreased curvature of the outer lens fibres with ageing.
• Index hyperopia It is due to cortical sclerosis. Index hyperopia occurs due to change in refractive index with age. It can be occurred in the diabetic patient.
• Positional hyperopia It may occur if the crystalline lens is being placed posteriorly. It may be occured by trauma or disease. It may occur as congenital anomaly.
• Aphakia Aphakia is the condition where the crystalline lens is dislocated from its anatomical position. Either it can be congenital or acquired. + 10 D lens is required for correction of aphakia. It is a high hypermetropic condition.
• Consecutive hyperopia
It happens due to surgically over corrected myopia or pseudophakia.
Functional hyperopia : It occurs due to paralysis
of accommodation as seen in patients with third Intracranial nerve palsy and internal ophthalmoplegia.
Oculomotor nerve (3rd nerve) palsy
Oculomotor nerve palsy is an eye condition resulting from damage to the third cranial nerve. This nerve controls 4 EOM except the lateral rectus and superior oblique.
In this condition, 3rd nerve’s palsy can impair eye movements, papillary reactions. These palsies can occur when pressure is put on the nerve or when the nerve does not get enough blood.
Internal ophthalmoplegia
It is a condition where limited involvement held to the papillary sphincter and ciliary muscle. It may be occured by a lesion in an
area of of the brain called the Medial Longitudinal Fasciculus (MLF). Generally multiple sclerosis and brainstem infarction are the reason of INO .
Symptoms :
I) Trouble focusing on nearby objects
II) Asthenopia ( Headache, eye strain, mild photophobia etc.)
III) Asymptomatic : Small error does not produce
any symptoms. It may be corrected
by patients’ accommodative effort.
Diagnosis : Diagnosis of hypermetropia
Clinical signs
I) Visual acuity: Visual acuity varies with degree
degree hyperopia and power of accommodation. Patients with low degree hyperopia may have normal visual acuity. In hyperopic patient, generally the visual acuity for seeing near objects.
Ii) Cover test : This test helps to diagnose
accommodative convergent squint. The better eye dominates for vision and the other eye develops accommodative convergent squint.
Iii) Eyelids: In an eyelid may develop
blepharitis,stye or chalazion.
Iv) Cornea : Cornea may be flatter (cornea plana)
V) Glaucoma : Due to increased size of the lens
with ageing, the eye becomes prone to an attack of narrow angle closure glaucoma.
Vi) Lens : Lens may be dislocated posteriorly
Vii) Fundus :In the fundus disc may be dark,
reddish color, irregular margins, confused with papillitis so termed as pseudopapillitis. Macula is situated further from the disc. We can see abnormal branchings of blood vessels.

Treatment:
I) Spectacles: Convex lenses are prescribed
E.g : +0.50 dsph/ +0.50 dcyl × 180°
Ii) Contact lense Contact lenses may be prescribed for cosmetic reasons. It may be given for unilateral hyperopia.
Iii) Visual Hygiene Visual hygiene is a term affectionately known as the 20-20-20 rule. This rule states that while reading or doing intensive near work, take a break about every 30 minutes.
Iv) Low Vision Aids
V) Surgery :
• YAG Laser Thermokeratoplasty
• Photorefractive keratotomy
• Conductive keratoplasty
• LASIK ( Laser assisted in Situ keratomileusis)
• Phakic intraocular lens
• Refractive lens exchange
Complications :
• Accommodative convergent squint
• Amblyopia
• Lid diseases
• Primary narrow angle glaucoma
Conclusion :
The close association between hyperopia, amblyopia & strabismus especially in children ,makes hyperopia, greater risk factor for more permanent vision loss than myopia.
The early diagnosis & treatment of significant hyperopia & its consequences can prevent a significant amount of visual disability in the general population.
References :
I) aimu.us/ hypermetropia
Ii) ncbi.nlm.nih.gov / Majumdar S, Tripathy K
Iii) researchgate.net / Dr. S.M. Payne
Iv) Visual science and Clinical Optometry by Dr.Bikas Bhattacharya
V) Wikigenes.org
Vi) slideshare.net / Hossein Mirzaie
Vii) slideshare.net / Suraj Shil







{kind=link}