
Vernal keratoconjuctivitis (VKC) is a recurrent, bilateral, external, ocular inflammation primary affecting boys & young adults living in warm, dry climates. It is an allergic disorder in which IgE & cell-mediated immune mechanisms play an important role. About three-quarters of patients have associated atopy & two-thirds have a family history of atopy. Such patients often develop asthma & eczema in infancy. The onset of VKC is usually after the age of 5 years and the condition eventually resolves around puberty, Only rarely persisting beyond the age of 25 years. VKC may occur on a seasonal basis, with a peak incidence over late spring & summer, although Many patients have Year round disease. Patients with VKC have a Higher incidence of keratoconus as well as other types of corneal ectasia such as pellucid marginal degeneration & keratoglobus.
The main symptoms are intense ocular itching which may be associated with lacrimation, photophobia, foreign body sensation & burning. Thick mucus discharge & ptosis also occur.
Demographics and Epidemiology:
VKC is a condition seen primarily in hot and dry climates most commonly in West Africa and the Mediterranean basin. It is also seen commonly in the Middle East, Japan, India, and South America. It is thought to be relatively unusual in North America and Western Europe. The increased incidence in hot regions is speculated to be secondary to a higher level of pollution by pollens and various other allergens. Males are affected more than females, but this difference becomes smaller as age increases. It is difficult to obtain an accurate prevalence as many patients may not present to clinics as they may have a mild form of the disease and the condition is largely self-limiting. Depending on region and climate, prevalence of VKC can vary widely. Additionally, prevalence in endemic regions is much higher when looking at adolescents compared to the population as a whole. For instance, one European study demonstrated the prevalence was between 1.2-10.6/10,000 At least one study exhibited a 4% prevalence in African schoolchildren The majority of VKC occurs in patients between the ages of 5-25 years old with an age of onset between 10-12 years old; however there are reports of patients as young as 5-months-old.
Pathophysiology:
A personal or family history of atopy is seen in a large proportion of VKC patients. VKC was originally thought to be due to a solely IgE mediate reaction via mast cell release. It has now been shown that IgE is not enough to cause the varied inflammatory response that is seen with VKC. Activated eosinophils are thought to play a significant role and these can be shown consistently in conjunctival scrapings; however mononuclear cells and neutrophils are also seen. Additional attention has been given to the CD4 T-helper-2 driven type IV hypersensitivity with immunomodulators such as IL-4, IL-5, and bFGF. Thought has been given to a possible endocrine method as well as there is a decrease in symptoms and prevalence after puberty.
A hereditary association has been suggested, but no direct genetic associations have been made. VKC is seen more often in patients who have atopic family histories, but no clear correlation with specific genetic loci has been elucidated.
The Three types are:
- Palpebral VKC
- Limbal VKC
- Mixed VKC
Limbal signs are more common in dark skinned races, while tarsal & corneal signs predominant in lighter-skinned races. It is, however, likely that many mild or atypical forms may be Unrecognized because no precise diagnostic criteria have been established. The long term prognosis is good.
Clinical feature :
- Palpebral VKC:
– Diffuse papillary hypertrophy,most marked on the superior tarsus.
– The papillae enlarge & have a flat topped polygonal appearance reminiscent of cobblestones.
– In severe cases, the connective tissue septa rupture, giving rise to giant papillae, which may be coated by copious mucus.
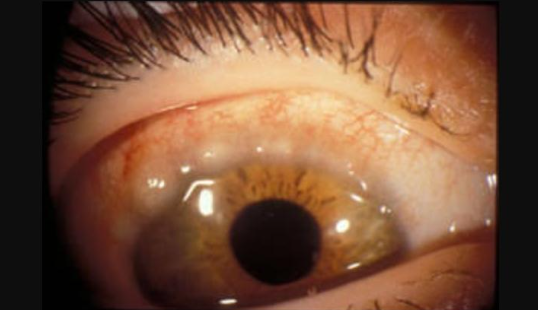
2.Limbal VKC:
Is characterized by mucoid nodules scattered around the limbus with discrete white superficial spots ( Tranters dots) Composed predominantly of eosinophils at the apices of the lesions.
3.Mixed VKC:
This has features of both the palpebral and limbal forms.
Differential diagnosis:
The main differential diagnosis to be considered is atopic keratoconjunctivitis (AKC). AKC typically has an older age of onset in the 2nd to 5th decade, as opposed to onset prior to age 10 with VKC. Conjunctival involvement is classically on the upper tarsus in VKC and on the lower tarsus in AKC. Additionally, AKC is typically more chronic in nature and more commonly results in scarring of the cornea and conjunctival cicatrization, whereas VKC is typically more self-limiting. Additional differential diagnoses to consider depending on history and physical would be seasonal allergic conjunctivitis and giant papillary conjunctivitis.
Treatment :
1.Topical:
- Antibiotic.
- Preservative free Lubricant.
- Steroid.
- Antihistamine.
- Supratarsal Steroid injection.
- Systematic
- Antihistamine.
- Antibiotics by mouth in severe cases.







{kind=link}