
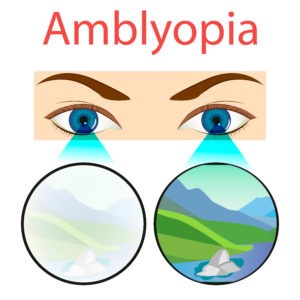
Amblyopia is the unilateral or rarely bilateral, decrease in best-corrected visual acuity (VA) caused by vision deprivation and abnormal binocular interaction, for which there is no identifiable pathology of the eye or visual pathway.
Amblyopia is produced by certain amblyopia factors operating during the critical period of visual development (birth to 6-7 years of age). During this period, the visual pathway continues to develop and the brain learns to interpret the signals that come from the eye. If for any reason, a young child cannot use one or both eyes normally, then the vision is not developed completely and the condition is called amblyopia. The most sensitive period for the development of amblyopia is the first six months of life and it usually does not develop after the age of 6-7 years.
CLASSIFICATION OF AMBLYOPIA:
- Strabismic Amblyopia.
- Stimulus Deprivation Amblyopia.
- Anisometropic Amblyopia.
- Isoametrtropic Amblyopia.
- Meridional Amblyopia.
FACTOR:
- Visual (from sense) deprivation occurs in anisometropia.
- Light deprivation, e.g due to congenital cataract
- Abnormal binocular interaction, e.g in strabismus.
- STRABISMIC AMBLYOPIA:
It results from prolonged uniocular suppression in children with a unilateral constant squint who fixates with the normal eyes. Squint is the most common cause of amblyopia.
- STIMULUS DEPRIVATION AMBLYOPIA:
It develops when one eye is totally excluded from seeing early in life as, in congenital or traumatic cataract, complete ptosis, and dense central corneal opacity.
- ANISOMETROPIC AMBLYOPIA:
It occurs in an eye having a higher degree of
refractive error than the fellow eye, It is more common in anissohypermetropic than the anisomyopic children. Even 1-2 D hypermetropic anisometropia may cause amblyopia while up to 3 D myopic anisometropic usually does not cause amblyopia. However, unilateral high myopia (>-6D) often results in serve amblyopia.
- ISOAMETROPIC AMBLYOPIA:
It is bilateral amblyopia occurring in children
With bilateral uncorrected high refractive error. Bilateral hyperopia >+5DS and myopia >-8DS are at risk of inducing bilateral amblyopia.
- MERTIDIONAL AMBLYOPIA:
It occurs in children with uncorrected astigmatic refractive error. It is selective amblyopia while bilateral meridional amblyopia is caused by bilateral astigmatism.
TERMOLOGY OF AMBLYOPIA:
Partial or complete loss of vision in one eye is caused by conditions that affect the normal development of vision.
These conditions include strabismus.
In amblyopia, the brain favors one eye over the other. The other eye is ignored. It is not adequately stimulated and the visual brain cells do not mature normally. Amblyopia is the most common cause of monocular blindness.
Treatment of strabismus may involve surgical correction of the eye muscle imbalance. In the case of severe refractive error, it should be corrected by glasses, contact lenses or if appropriate, Lasix wearing an eye is a hallowed treatment for amblyopia. Another option is atropine eye drops to blur the vision temporally in the stronger eye. Weekend atropine provides an improvement in visual acuity of a magnitude similar to that provided by daily atropine in treating moderate amblyopia.
People of all ages, including adults, can be treated for amblyopia, commonly referred to as “Lazy Eye”. For the same, this is shocking news. That’s because there’s been a pervasive and long-held misconception in the general public, and even the scientific and medical communities, that anyone older than eight can’t be treated effectively for lazy eye.
As development optometrists, we are here to all you that this generalization is just not accurate. It is possible for adults to be treated for lazy eyes.
In most cases of amblyopia, one eye just isn’t seeing as clearly as the other.
Normally, the brain receives two images at slightly different angles, and it combines them to produce a 3D image. This is called binocular vision. But that’s not the case with amblyopia.
The suppression of information from one eye negatively impacts the development of binocular vision. As a result, it seems like one eye does all the work of seeing. Thus’ the other eye is characterized as “Lazy.”
Amblyopia in adults can be treated, often through a combination of the prescription lens, vision therapy, and sometimes patching. More on that below. But first, let’s address the misconception that treatment can only work with young children.
Amblyopia or lazy eye is a visual development disorder in which the vision through one eye fails to develop properly in early childhood. It manifests as a reduced vision in one or both eyes that is not correctable by glasses, contact lenses, or eye surgery. A most important fact about amblyopia- Amblyopia or lazy eye fails to work not because it’s lazy but because it’s actively inhibited by the follow, sighted eye.
In Amblyopiaa not only the visual acuity but also-
- Visual performance is affected.
- Reading is affected.
- Eye-hand coordination is affected.
- Depth perception is affected.
- Spatial judgment is affected.
At Artificial Eye Co we work on all these parameters to bring back visual acuity along with binocularity, eye-hand coordination, depth perception, and spatial judgment is also improved at the end of the treatment. Computerized and non-computerized treatment is done to get the best result in the shortest time.
At first, we do the best possible spectacle or contact lens correction. Then the visual acuity is checked and active vision therapy is done to improve binocularity. Our unique treatment is based on vision therapy and we work on improving vision for near, intermediate, and distance. We not only train your eyes but also your brain to see better. We have special treatment plans for people who don’t want to occlude or put drops to blur the eye. The patient needs to come to our center for the treatment where we train the eye and the brain to improve the vision and binocularity.
If you are an adult and sufferings from amblyopia.
- Throwing catching or hutting a ball.
- Driving and parking a car.
- Planning and building a 3D object.
- Difficulty in sewing and threading a needle.
- Reaching out to shake someone’s hand
- Pouring into a container.
- Climbing stairs.
- Difficulty in reading- The letters spill over into one another and crowd one another out.
Treatment is directed to the cause and maybe surgical removal of the obstruction, correction of the drooping eyelid, cataract surgery, eyeglasses, contact lenses, etc. The earlier the treatment is begun, the faster the correction. Often the child has to wear an eye patch on the GOOD eye or use eye drops to blur it, forcing the use of the eye with the decreased vision. We used to believe that this treatment had to be done by the age of seven years but often can work in older children.
Pleoptics and flashing light treatment have no proven value. Laser vision correction has been used to corrected has been used to correct the refractive errors, but patching is still necessary. The important message here is that no child is too young to have an eye examination, and parents should consult an ophthalmologist promptly if they notice or suspect anything or if there is a family history of amblyopia.








{kind=link}