

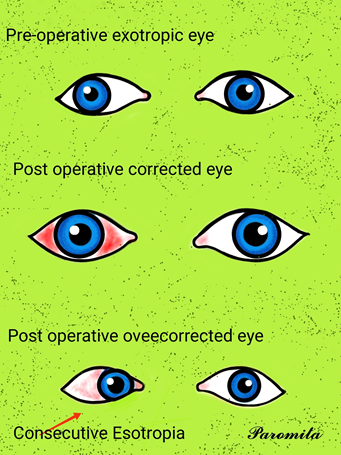
Definition : This is a type of convergent strabismus that occurs due to poor vision in one eye. There are various causes of poor vision including problems with the retina or optic nerve, either present from birth or developed in later life. Consecutive esotropias refer to a convergent strabismus that has developed following surgery for an exotropia. This is relatively rare but can happen following surgery for an intermittent distance exotropia (IDEX). It has been reported to occur under following two clinical situations :
Surgical overcorrection of exotropia, is the cause of consecutive esotropia in almost all the cases.
- Very large overcorrection with gross limitation of ocular motility noted on the very next day is possibly due lost or slipped lateral rectus muscle. Under such circumstances, patient should undergo surgery again within 24 hours.
- Small to moderate (10∆ to 50∆) overcorrection needs to be managed depending upon the age of the patient :
- In adults (visually mature patients), as describe earlier, an overcorrection of 10∆ to 20∆ is desirable to ultimately achieve stable results If overcorrection is more than 20∆ after at least six weeks of surgical measures should be tried during the wait and watch period of 6 months. Re refraction should be done and if hypermetropia is detected, it should be fully corrected. Bifocals or mitotic therapy may be prescribed, if near esotropia is more than the distance. Prismotherapy in the form of fresnel membrane prism that fully correct the deviation should be prescribed. The prism power should be adjusted monthly depending upon the latest examination results. Re surgery is indicated in patiens where overcorrection of more than 20∆ continues even after the above described non surgical therapy for a period of 6 months.
It has been recommended that in planning second surgery cooper’s dictum( i. e. The decision about choice and amount of surgery should be made as if the present patient is a fresh case of squint) should be followed.
- In small children (i. e. Visually immature patients), as stated earlier, the consecutive esotropia is associated with a greater danger of developing monofixation syndrome and suppression amblyopia. So these patients need a special care. Following measures should be taken within 2 weeks of the surgery.
. Re refraction should be done and any hypermetropic error should be fully corrected.
. Bifocals or miotics should be prescribed, if the deviation is greater at near.
. occlusion therapy. Initially, when there is no fixation preference, alternate occlusion should be done for a few weeks. If the child develops moderate fixation preference, conventional occlusion of the preferred eye should be used till either there occurs alternate fixation or only a mild fixation preference.
. prismotherapy in the form of ‘press on’ baseout fresnel membrane prism should be started at this stage to maintain bifoveal fixation. The prism power should be fully correct the deviation and be adjusted monthly depending upon the latest examination results.
. Re surgery indicated, if the child remains oveecorrected by 15∆ or more in spite of the above described non surgical therapy.
For re operation, the cooper’s dictum should be followed.
Methods: We retrospectively reviewed the medical records of 526 patients who had undergone exotropia surgery. We evaluated the risk factors for consecutive esotropia, defined as esodeviation ≥ 10 prism dioptres (PD) at postoperative month 1 or later. We also evaluated the clinical course of consecutive esotropia with non-surgical and surgical management.
Results : Consecutive esotropia occurred in 26 (4.94%) of 526 patients. Divergence excess type of exotropia (p=0.036), amblyopia (p=0.046), bilateral lateral rectus recession (p=0.008), esodeviation of ≥ 20 PD at postoperative day 1 (p=0.000), younger age at diagnosis and surgery (p=0.010, p=0.003) and shorter duration from onset to surgery (p=0.039) showed significant association with consecutive esotropia. Among 26 patients, 15 became orthophoric with full-time patching ± Fresnel prism glasses. Eleven patients failed to show improvement of the esodeviation with non-surgical management; seven of these underwent surgery for sustained esotropia. Among these patients, five showed orthophoria at the final follow-up.
Conclusion : Divergence excess type, bilateral lateral rectus recession, amblyopia, younger age at diagnosis and surgery, shorter duration from onset to surgery and overcorrection of ≥ 20 PD at postoperative day 1 were predisposing factors for consecutive esotropia. In less than half the consecutive esotropia patients (11/26), esodeviation persisted with non-surgical management. Surgery for consecutive esotropia showed relatively favourable outcomes.







{kind=link}