
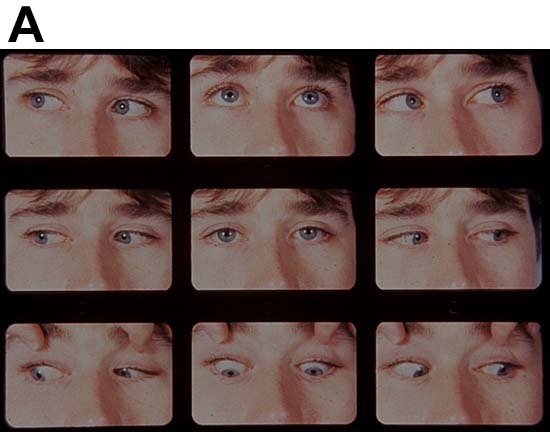
CONVERGENCE : convergence is a disjugate movement of the eyes in which both eyes rotate inward so that the lines of sight intersect in front of the eyes. It allows bifoveal single vision to be maintained at any fixation distance. Convergence remains more or less same throughout life. It does not deteriorate with increasing age as does accommodation, but may deteriorate in certain abnormal conditions. The power of convergence can be increased by orthoptic exercises.
Stimulus of convergence :
1) Proximity of the object
2) Accommodation
3) It can be voluntary
TYPES OF CONVERGENCE
- Voluntary convergence
- Reflex convergence
Voluntary convergence is convergence of of visual axes which can be produced at will. It is not a part of everyday vision.
Reflex convergence is the convergence of visual axes which is not under complete voluntary control. It has 4 components
- Tonic convergence : is convergence that results from some inherent innervational tone of extra ocular muscles when a person is awake. It is a convergence which determines the position of visual axis in relation to each other and is primarily responsible for maintaining the eye in primary position. it is independent of fusion or object proximity.
2)Fusional convergence : is the amount of convergence required to maintain fusion. It is the convergence produced to ensure that similar retinal images are onto corresponding retinal areas. It occurs without a change in refractive status of the eye.
3)Accommodative convergence : occurs when eyes accommodate that is with stimulus of accommodation. The stimulus of convergence here is blurred retinal image .
- Proximal convergence : it is stimulated by the perception of the position of an object of attention and is independent of accommodation.
CONVERGENCE PATHWAY: Afferent impulses from internal rectus muscle are passed along with third nerve to mescencephalic route of the 5th nerve to the nucleus of perlia next to edinger westphal nucleus. on both sides from EWN the efferent impulses are carried via the motor fibres of the 3rd nerve to the accessory ciliary ganglion next to sphincter pupillae.
Units of measuring convergence :
Angle of convergence : is an angle that is formed between the primary lines of sight during convergence. Its size depends on fixation distance and IPD becoming smaller with increasing distance of fixation object and becoming larger with increasing IPD. It can be measured in meter angle, prism dioptre or degree.
Near point of convergence : is the closest point at wich an object can be seen clearly during bifoveal vision.
Far point of convergence : refers to relative position of the eyes when they are completely at rest.
Range of convergence : is the distance between far point of convergence and NPC. The part of the range of convergence between the eye and infinity is called positive convergence and the part beyond infinity (behind the eye) is called negative convergence or divergence .
Amplitude of convergence : refers to difference in the convergence power exerted to maintain the eye in a position of rest and in a position of maximum convergence.
AC/A ratio : is the relationship between accommodative convergence (AC),expressed in prism dioptres, and accommodation (A),expressed in lens dioptres. The relationship is linear one and is thought to be stable throughout life. The normal AC/A ratio is about 3-5 prism dioptres for 1 dioptre of accommodation.
Anomalies of convergence :
1)convergence insufficiency : is the inability to obtain and or maintain adequate binocular convergence for any length of time without undue effort.
2)convergence insufficiency associated with accommodative insufficiency
3)convergence paralysis
4)convergence spasm
CONVERGENCE PARALYSIS : it refers to the total lack of ability to overcome any amount of baseout prism. It occurs secondary to some organic diseases of the brain or the nucleus of 3rd cranial nerve.
CLINICAL FEATURES :
- Convergence is completely absent
- Exotropia and crossed diplopia on attempted near fixation only
- Adduction is normal
- Accommodation is usually normal but in some cases it may br reduced or absent
DIAGNOSIS: Bielchowskey’s criteria for diagnosis of convergence paralysis include,
- Evidence of intracranial disease
- H/O sudden onset of crossed horizontal diplopia at near fixation
- Reproducible findings on subsequent examinations
- Preservation of accommodation and papillary reaction on attempts to converge
Differential diagnosis :
Convergence paralysis can be differentiated from functional convergence insufficiency by use of base out prisms. A patient with convergence paralysis will immediately have diplopia , while in convergence insufficiency several dioptres of convergence amplitude can be demonstrated.
TREATMENT
- Base in prisms are prescribed at near to alleviate the diplopia at near.
- Plus lenses with base in prisms may be required in patients having weakness of accommodation.
- Occlusion of one eye at near may be indicated in patients where it is not possible to restore comfortable single binocular vision.
- Eye muscle surgery is contraindicated in this condition.
By SYEDA SALMA (B.optom)
References: Theory and practice of optics anf refraction by AK khurana
Binocular vision and ocular motility (von nordan)








{kind=link}