
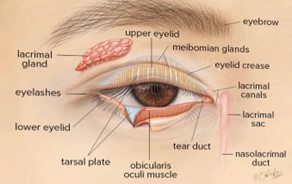
An eyelid is a thin fold of skin that covers and protects an eye. There are upper and lower eyelids. Many things can affect the eyelids or are related to the eyelid.
Eyelids can be found in other animals, some of which may have a third eyelid, or nictitating membrane. A vestige of this in humans survives as the plica semilunaris. Its key function is to regularly spread the
tears and other secretions on the eye surface to keep it moist, since the corne must be continuously moist. They keep the eyes from drying out when asleep.
Moreover, the blink reflex protects the eye from foreign bodies. The eyelashes are hairs that grow on the edges of the upper and lower eyelids. The lashes are short (upper lashes are typically just 7 to 8 mm in length) hairs, though can be exceptionally long (occasionally up to 15 mm in length) and prominent in some individuals with trichomegaly. These hairs known as lashes grow from the upper and
lower eyelid margins to further protect the eye from dust and debris.
STRIATED MUSCLE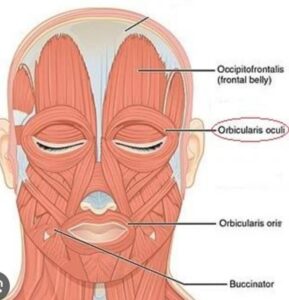
Orbicularis oculi – Main protractor of eyelid
• Innervated by cranial nerve 7
• Divided into three parts:
1. Pretarsal
2. Preseptal
3. Orbital – Forced eyelid closure
Pretarsal part
Superficial origin-MCT
Deep origin – post lacrimal crest
Deep heads fuse near common canaliculus to form Horners muscle (Pars lacrimalis) Contraction of which draws the eyelids medially and posteriorly. The resulting lateral pull creates a negative pressure in the lacrimal sac and draws the tears from the canaliculi into the sac.
• Preseptal part arises from MCT medially a forms Lateral palpebral raphae laterally
• Orbital portion arises from MCT, frontal bone, maxillary bone – fibres form a ellipse
and insert below origin
• Near eyelid margin fibres of pretarsal part –Muscle of Riolan (pars ciliaris) – creates gray line, plays a role in meibomian glandular discharge, blinking and position of eyelashes
LPS – The levator palpebrae superioris originates from inferior surface of the lesser wing of the sphenoid bone, just above the optic foramen. 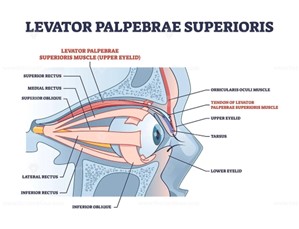 It broadens and decreases in thickness (becomes thinner) and becomes the levator aponeurosis. This portion inserts on the skin of the upper eyelid, as well as the superior tarsal plate. It is a skeletal muscle. The superior tarsal muscle, a smooth muscle, is attached to the levator palpebrae superioris, and inserts on the superior tarsal plate as well. The Levator palpebra superioris is described with the anatomy of the eye. The Orbicularis oculi is a broad, flat, elliptical muscle which occupies the eyelids or palpebrae, surrounds the circumference of the orbit, spreads over the temporal region, and downwards on the cheek. It consists of three main portions-orbital, palpebral and lacrimal.
It broadens and decreases in thickness (becomes thinner) and becomes the levator aponeurosis. This portion inserts on the skin of the upper eyelid, as well as the superior tarsal plate. It is a skeletal muscle. The superior tarsal muscle, a smooth muscle, is attached to the levator palpebrae superioris, and inserts on the superior tarsal plate as well. The Levator palpebra superioris is described with the anatomy of the eye. The Orbicularis oculi is a broad, flat, elliptical muscle which occupies the eyelids or palpebrae, surrounds the circumference of the orbit, spreads over the temporal region, and downwards on the cheek. It consists of three main portions-orbital, palpebral and lacrimal.
Orbicularis Oculi
The orbicularis oculi muscle has three distinct parts palpebral, lacrimal and orbital.
• Attachments – Originates from the medial orbital margin, the medial palpebral ligament, and the lacrimal bone. It then inserts into the skin around the margin of the orbit, and the superior and inferior tarsal plates.
• Actions:
1. Palpebral part – gently closes the eyelids.
2. Lacrimal part – involved in the drainage of tears.
3. Orbital part – tightly closes the eyelids.
• Innervation – Facial nerve (CN VII, temporal and zygomatic branches) The lateral palpebral raphe Is a much weaker structure than the medial palpebral ligament, It is formed by the interlacing of the lateral ends of the palpebral fibers of the Orbicularis oculi, strengthened on its deep surface by the orbital septum. A few lobules of the lacrimal gland lie between it and the more deeply placed lateral palpebral
ligament (Whitnall).
• Whitnalls ligament is an important surgica landmark – easy to see intraoperatively as a strong white band of fibrous tissue
• Generally tissue superior to ligament is muscle while inferior is aponeurosis
• Courses forward as Muscular portion for around 40mm then descends vertically and fans out as an aponeurosis around 15mm long
NON STRIATED MUSCLES
• Mullers muscle originates on undersurface of Laponeurosis, inserts along upper eyelid superior tarsal margin sympathetically innervated smooth muscle
• Provides approx 2mm elevation to upper lid
• If interrupted – eg HORNERS SYNDROME – mild ptosis ensues
• Peripheral arterial arcade is found b/w Lps aponeurosis and Mullers ms – this vascular arcade serves as a surgical landmark to identify Mullers muscle
• The superior tarsal muscle (muscle of Müller) is composed of smooth muscle and originates on the posteroinferior aspect of the levator muscle
• These smooth muscle fibers begin to appear within the striated muscle at the point at which the muscle becomes aponeurotic
• The superior tarsal muscle inserts on the superior edge of the tarsal plate.
• Contraction of Müller’s muscle can cause an added 2 mm of lid elevation.







{kind=link}