
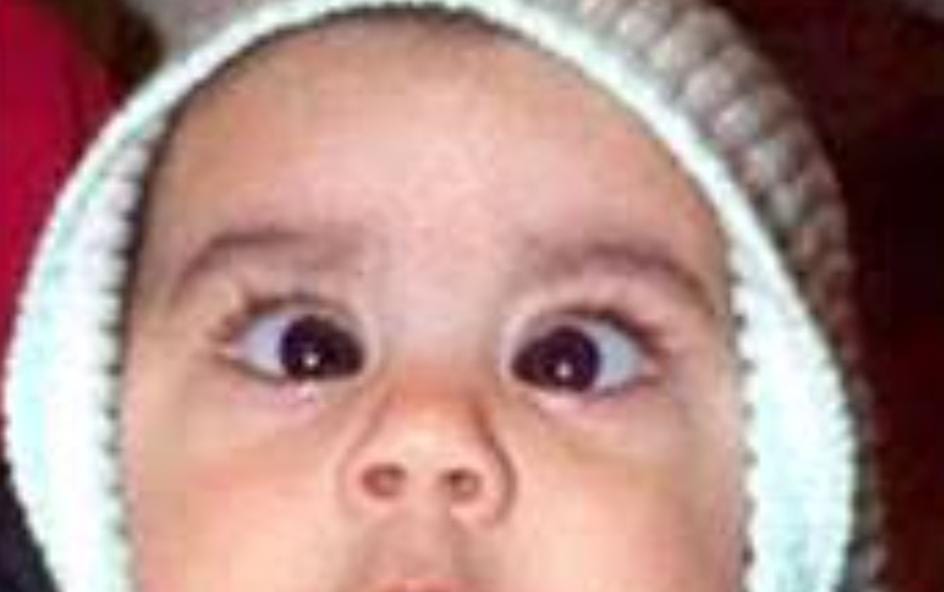
Exotropia is a type of strabismus it’s misalignment of the eye. In which one or both eyes rotate outward. This condition can start in the first few months of life or at any time during childhood.
Exotropia may appear at birth or later in life. It can usually be managed or treated, but will vary depending on the type and severity of the treatment.
Types of exotropia:
This condition of the eye can be congenital (present at birth) or acquired (developing in childhood).
There are three types of acquired exotropia:
Non-stop exotropia, which occurs occasionally.
Sensitive exotropia, which occurs in the eye with impaired vision and turns it outward.
Persistent exotropia, which may develop after surgery for the treatment of crossed eyes.
Congenital Exotropia :
Congenital exotropia is also called infantile exotropia. People with this disease tend to roll their eyes or eyes externally from birth or childhood.
Causes :
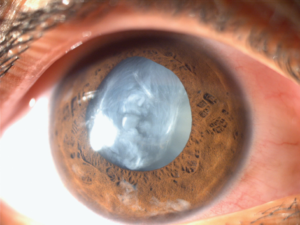
Exotropia occurs when there is an imbalance in the eye muscles or a signal problem between the brain and the eyes. Sometimes a health condition, such as cataract or stroke, can occur. The condition can be inherited.Exotropia can be seen in children with very poor eyesight or some genetic disorder that affects the eyes. It can also occur with previous eye muscle surgery for 3rd cranial nerve palsy or strabismus.
Testing and diagnosis :
Measure visual acuity in each eye and both eyes together
Cycloplegic refraction
External or slit lamp test
Fundus (retina) examination
Complete eye examination
Diagnostic imaging, including MRI scans, to determine if there is a defect in the eye due to nerves rather than muscle problems.
Genetic studies to identify chromosomal problems that may indicate genetic syndrome.
Risk factors :
Positive family history of Strabismus, amblyopia, childhood cataracts, or glaucoma.
Some genetic disorders that affect the eyes.
Some eye disease like Pediatric cataract, glaucoma.
Symptoms:
Decreased vision.
Depth perception decreases.
External deviation of the eye, often at first occasionally.
Sensitivity to bright light and close eye.
One or both eyes are rolling outwards.
To much eye rubbing.
Winking or covering one’s eyes when looking at bright light or trying to see distant objects.
Eye strain during near work
Unable to read properly because of divergent eye
Management :
CONGENITAL EXOTROPIA
Congenital exotropia is extremely rare. Congenital exotropia may occur in patients whose are systemic disease, craniofacial anomalies, ocular albinism, or cerebral palsy. The treatment for congenital exotropia is bilateral lateral rectus recessions, which should be performed after 6 months of child’s age. This syndrome should not be confused with the normal, variable, small-angle exodeviation seen in normal new borns. Instead, congenital exotropia is a large-angle constant exodeviation, with a relatively poor prognosis for fusion. It has a much higher incidence of amblyopia than intermittent exotropia, with the incidence of amblyopia being similar to congenital esotropia.
Surgical criteria may vary slightly, but surgery is usually indicated when exotropia is frequently present, when the patient experiences significant symptoms ( double vision, squinting), or when there is evidence that the patient is losing binocular vision. Surgery may not be recommended if exotropia is adequately controlled by spectacles or other non-surgical procedures.
Part-time occlusion: Non-deviating normal eye partial time obstruction can treat deformed eye suppression and amblyopia and thereby correct exotropia and bring it back to exophoria. In the case of showing equal priority, eye alternatives may be blocked. Part-time blockade has been found to be effective in very young children.
Use of prisms: Base-in prisms apply bifocal stimulation and help relieve eye strain. Prisms can be used to improve fusion control.
Conclusion:
Infantile exotropia is rare. However, as in patients with infantile isotropia, patients with exotropia may be expected to have better visual acuity but unstable eye alignment. Also, u early onset isotropia, although surgical intervention is usually required, high levels of binocular function develop in some patients with exotropia.
If your child has eye misalignment, you need to see an ophthalmologist.
The child should be given proper treatment.







{kind=link}