

“Early optical correction in children isn’t just about clarifying vision—it’s about nurturing
healthy eye development and preventing complications.” – Sorot Wutthiphan, MD
Optical correction in children is a nuanced and critical aspect of pediatric eye care. Beyond
simply providing clear vision, well-considered prescriptions are essential for preventing
complications like amblyopia, strabismus, and other developmental visual issues. In young
children, early corrective measures can help manage refractive errors like hyperopia,
myopia, and astigmatism, each of which has unique developmental patterns and risks if left
uncorrected. In this blog, we’ll delve into Dr. Sorot Wutthiphan’s guidelines, exploring how
to approach refractive errors in children while supporting
Key Aspects of Eye Development and Refractive Correction in Childhood
Emmetropization and Eye Growth:
During infancy and childhood, the eye undergoes natural changes through
emmetropization, moving from high refractive errors to near-normal vision. This process
involves the eye lengthening and the cornea and lens flattening, which helps many children reach low refractive states without correction. However, certain conditions like high
hyperopia (> +5.00 D) may require early intervention to avoid risks such as amblyopia (lazy
eye) and strabismus (misalignment). [1]
Hyperopia and Myopia: Prescription Guidelines
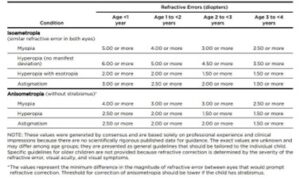
Figure 1: AAO Guidelines For Prescribing Spectacles in Pediatrics
Image courtesy: American Academy of Ophthalmology. (n.d.). Table 3: 11.8.17. Retrieved December 29, 2024, from
https://www.aao.org/Assets/e27390d7-f46d-4122-a1c8-41e4ce045811/636458251660630000/table-3-11-8-17-pdf
The American Academy of Ophthalmology (AAO) guidelines recommend prescribing
spectacles for preschool-aged children with myopia of -5.00 diopters or more, hyperopia of
+6.00 diopters or more without strabismus, or astigmatism of 3.00 diopters or more. For
school-aged children, glasses should be prescribed if myopia, astigmatism, or hyperopia
without esotropia results in a visual acuity of less than 20/30. Additionally, anisometropia
should be corrected to within 1 diopter difference between the two eyes. [4]
Hyperopia (Farsightedness):
Mild hyperopia often reduces naturally through emmetropization, but high hyperopia (>
+3.50 D) can cause blurred vision, amblyopia, or strabismus if uncorrected. In such cases,
full correction is usually prescribed, especially with strabismus. In very young children,
partial correction might be considered to allow natural refractive adjustment. [1]
Myopia (Nearsightedness):
Myopia typically emerges later in childhood and progresses during school years. Full
correction is often prescribed for moderate to high myopia in older children to ensure clear
distance vision. Low myopia in younger children may be monitored initially. Regular check-
ups are essential since untreated myopia can progress. Treatments to control progression
include cycloplegic agents, plus lenses, and rigid contact lenses. [1]
Astigmatism, Anisometropia, and Amblyopia Risks:
Uncorrected astigmatism over 2.50 D or anisometropia (unequal refractive error) increases
the risk of amblyopia. Even a small difference (e.g., 1.00 D in hyperopia or 3-4 D in myopia)
can lead to amblyopia. Full correction is recommended in these cases to prevent visual
impairment. [1]
Special Considerations for Preterm Infants:
Preterm infants may have higher myopia and astigmatism, normalizing if no retinopathy of
prematurity (ROP) is present. With ROP, refractive errors often persist due to disrupted
emmetropization. [1]
Guidelines for Optical Correction:
Cycloplegic Refraction is crucial in young children to ensure accurate assessment by relaxing
accommodation.

Table 1 : Guidelines for using of Cycloplegics according to Age and Refractive needs
[ Table Courtesy : AK Khurana [2009]. Theory and practice of Optics and Refraction, Table 5.1 , page 136 ]
Refraction Differences Among Cycloplegic Agents:
Atropine: Provides the most complete cycloplegia, ideal for detecting latent hyperopia
in children.
Cyclopentolate: Ensures effective cycloplegia with faster onset and shorter duration
than atropine, suitable for routine exams.
Tropicamide: Has the shortest cycloplegic effect, potentially insufficient for patients
with high accommodation.
General Side Effects:
Ocular: Blurred vision, photophobia, increased IOP, and allergic reactions.
Systemic: Dry mouth, flushing, tachycardia, urinary retention, and rare CNS effects like
confusion in pediatric/geriatric patients. [3]
Amblyopia and Strabismus Treatment involves early correction combined with therapies like
occlusion.
Myopia Control Interventions include low-dose atropine, orthokeratology, and lifestyle
changes to reduce close-up tasks, which have shown success in slowing myopia
progression. [2]
As optometrists, the clarity we provide extends beyond the lenses we prescribe; it shapes a
child's world, fueling their learning, exploration, and growth. By understanding and applying
the essentials of pediatric optical correction, we are not just correcting vision—we are
fostering confidence and potential in each young patient. Let us continue to guide and
inspire the vision of the next generation, one clear lens at a time.
References:
[1] Suchoff, I. B., & Ciuffreda, K. J. (2004). A primer for the optometric management of
unilateral spatial inattention. Optometry (St. Louis, Mo.), 75(5), 305–318.
[2] Porter, D. (2024, September 24). Myopia control in children. American Academy of
Ophthalmology. https://www.aao.org/eye-health/diseases/myopia-control-in-children
[3] Wakayama, A., Nishina, S., Miki, A., Utsumi, T., Sugasawa, J., Hayashi, T., Sato, M., Kimura,
A., & Fujikado, T. (2018). Incidence of side effects of topical atropine sulfate and cyclopentolate
hydrochloride for cycloplegia in Japanese children: a multicenter study. Japanese Journal of
Ophthalmology, 62(5), 531–536. https://doi.org/10.1007/s10384-018-0612-7
[4] American Academy of Ophthalmology. (n.d.). Table 3: 11.8.17. Retrieved December 29,
2024,from https://www.aao.org/Assets/e27390d7-f46d-4122-a1c8-
41e4ce045811/636458251660630000/table-3-11-8-17-pdf








{kind=link}