
Introduction
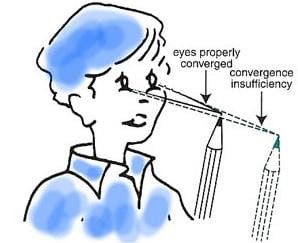
Convergence insufficiency (CI) is a common binocular vision disorder that can significantly impact reading and other near-vision activities. Often undiagnosed in routine eye exams, this condition manifests as difficulty or discomfort when trying to focus on close objects, leading to symptoms like eyestrain, headaches, and even double vision. As the digital age increases demands on near vision, diagnosing and managing convergence insufficiency is essential for maintaining visual comfort and efficiency in daily activities which enhances the quality of vision, productivity as well as the quality of life. In this blog we are going to understand in detail about the fundamentals of CI, its causes, sign, symptoms and treatment strategies in a concise and professional manner. Etiology: What Causes Convergence Insufficiency?
The causes of CI can be broadly categorized into primary (functional) and secondary (organic) origins:
1. Primary or Idiopathic Causes:
o Anatomical factors: Wide interpupillary distance can predispose individuals to CI.
o Functional Development: Delayed or inadequate development of convergence mechanisms is a
significant factor.
o Precipitating causes: illness, ocular fatigue (tiredness) from prolonged near work and poor
lightning, advancing age, drugs and pregnancy
2. Secondary (organic) Causes:
o Neurological Conditions: Disorders such as multiple sclerosis, Parkinson's disease, and traumatic brain injuries can impair the convergence mechanism.
o Systemic Illnesses: Viral encephalopathies, diphtheria, or infectious mononucleosis can contribute to secondary CI.
o Ocular Disorders: Uncorrected refractive errors like high myopia or hypermetropia (more than 5 diopters) may exacerbate the condition due to insufficient accommodative-convergence mechanisms.
3. Lifestyle Factors: o Increased screen time, poor posture can strain convergence systems, leading to insufficiency.
Symptoms: Recognizing the Signs
Symptoms of CI primarily emerge during near-vision tasks and may include:
Visual discomfort: Eyestrain and headaches, sensation of tension, particularly after extended reading or
screen use
Fatigue: Sleepiness or loss of comprehension during reading
Blurred or double vision: Particularly noticeable when focusing on close objects. Individuals can see
crowded or double image.

Difficulty concentrating: A tendency to avoid near-vision tasks due to discomfort. Difficulty in
changing focus from distance to near.
Diagnosis
The diagnosis of CI typically involves:
Near Point of Convergence (NPC) Testing: Assessing the closest point where binocular single vision
can be maintained. Receded NPC, more than 10 cm from the baseline.
Cover Test: Exophoria at near, orthophoria or low exophoria at distance.
AC/A ratio: low
Fusional Vergence Testing: Measuring the eyes' ability to maintain single vision using prisms. Low
positive fusional vergence (low base out prism)
Binocular accommodative facility: fails or having difficulty in clearing the +ve (convex) lens
Low negative relative accommodation (NRA)
Treatment Strategies (Management)
1. Correct the refractive error by suitable lens: Optimal lens refraction
2. Vision Therapy
Phase1: Build good communication and relation with the patient. Start session with accommodative
therapy because CI is often associated with accommodative anomalies. The early session can be started
with accommodative and peripheral stereo enhancement which include loose monocular accommodative
rock, near-far Hart chart, brock string and pointer in the straw etc.
Phase2: The accommodative anomalies and peripheral stereopsis are developed in the phase1, the
phase2 progresses from peripheral to central stereopsis. In this phase we try to eliminate the gross
suppression (if present) and to increase the positive fusional vergence (PFV) at near with the help of
vectograms, stereograms, tranaglyphs etc.
Phase3: Flat fusion is introduced with anti-suppression. Techniques used in this therapy are aperture
rule, life saver cards, anti-suppression, eccentric circles, cheiroscopic tracing etc.
Phase4: In this phase we concentrate on both convergence and accommodation flexibility. We add the
accommodative flipper with tranaglyphs, aperture rule, life saver card and vectograms to achieve normal
both accommodative and vergence demand
3. Prisms:
o Base-in prisms may be used as a temporary measure to alleviate symptoms by reducing the
demand on convergence (should be avoided in children)
4. Surgical Intervention:
Surgery is rarely indicated and reserved for extreme cases where significant exophoria or esotropia at
near fixation persists despite comprehensive non-surgical management. Procedures like medial rectus
resection may be considered
5. Lifestyle Adjustments:
o Encouraging breaks during prolonged near tasks to reduce visual fatigue.
o Maintaining proper posture and lighting conditions during reading or screen use







{kind=link}