
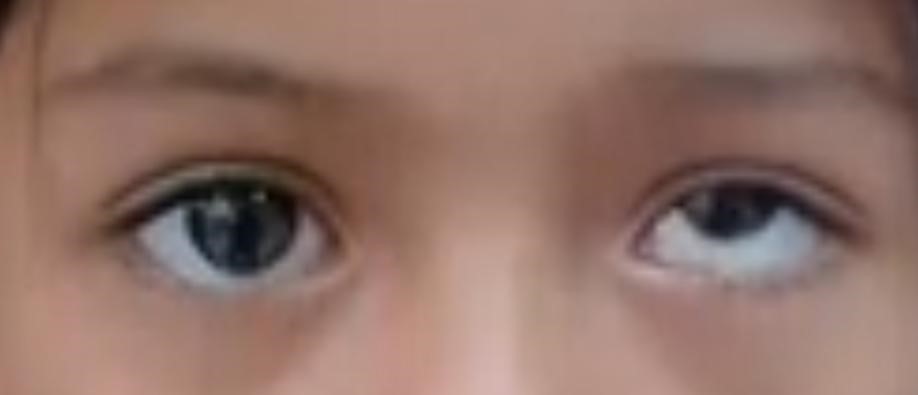
- Vertical Strabismus refers to a vertical misalignment of the visual axes of the two eyes in the vertical direction in any of the nine cardinal positions of gaze.
- Vertical Strabismus is more symptomatic than horizontal Strabismus.
- Usually, the vertical recti or the oblique muscles are involved.
- This could be Comitant (Deviation that is the same magnitude regardless of gaze position) or Incomitant (it’s magnitude varies as the patient shifts his or her gaze).
- Associated with horizontal deviation.
- Types are—
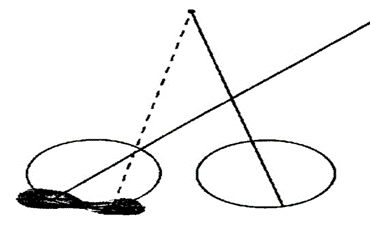
▪︎Hypertropia:– non Fixating eye is higher than Fixating eye.
▪︎Hypotropia:– Fixating eye is higher than non Fixating eye.
CLASSIFICATION OF VERTICAL STRABISMUS :
- Depending upon the constancy of deviation hyperphoria
- Intermittent Hypertropia
- Hypertropia
- The direction of deviation in the non Fixing eye
- Hypertropia
- Hypotropia
- Depending upon the competence of deviation
- Comitant vertical deviation
- Refractive (induced)
- End result of long-standing Paralytic deviation
- Incomitant vertical deviation
- Apparent oblique muscle dysfunction interior oblique overaction Inferior oblique Underaction Superior oblique overaction Superior oblique Underaction
- Paretic vertical deviation Congenital unilateral Superior oblique paresis-congenital Superior oblique paresisBilateral Superior oblique paresisMonocular Elevation deficiency Monocular depression deficiency Superior rectus paresis Inferior rectus paresis Skew deviation
- Restrictive vertical deviation-
- Vertical deviations in Duane’s retraction syndrome. Brown’s syndrome Congenital muscle fibrosis Dysthyroid orbitomyopathy.Post-traumatic orbital wall fractures.Tumors, pseudotumors, and cysts in the orbit.
- Dissociated vertical deviation (DVD)
- Monocular DVD
- Binocular or alternating DVD
ETIOLOGY :
- Convertion of Incomitant Paralytic hyperdeviation.
- Ocular muscle weakness
- Central ocular control disturbances
- Underaction of extraocular muscles.
- Secondary to hemorrhage or mechanical trauma with extraocular muscle atrophy.
- Traumatic neuroparesis.
- Secondary fibrosis of the extraocular muscles.
- Unequal refractive correction.
CLINICAL FEATURES :
Signs:‐
Common signs include —
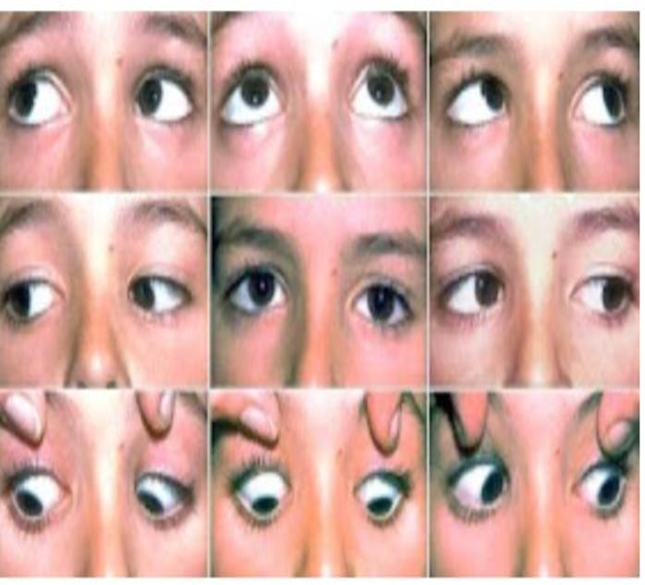
- Ocular deviation in the vertical direction in any of the nine cardinal positions of gaze position of gaze with either eye fixing on the Hirschberg test and prism cover test.
- Ocular motility tests can show the limitation of movements in the vertical direction.
Symptoms:‐
- Commonly Intermittent than constant.
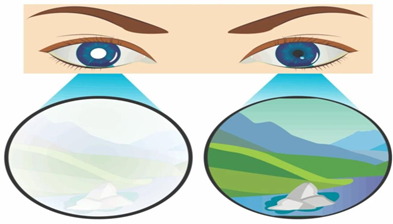
- Suppression
- Vertical Diplopia
- Amblyopia
- Vertical anomalous retinal correspondence
- Vertical deviation of the eye.
- Abnormal head posture – Tilting of head and chin up or down.

- Repeated measurement shows the overaction of one or more cyclovertical muscle.
TREATMENT :
- Orthotics:—
- to eliminate suppression may be indicated prior to surgery.
- It is impossible to improve Vertical fusional vergence through Orthotic training.
- Prismotherapy:—
- Smaller than 11D can correct prism
Hypertropia = 5pd BD
Hypotropia = 5pd BO
- Surgical correction








{kind=link}